
Remember me




In the survey of the senior physicians of German child and adolescent psychiatric facilities, a total of 55 calls were documented. Of these, 49 individuals initiated the survey, and 73.5% (n = 36) of them completed the questionnaire in its entirety. During the survey period for the architect-specific inquiry, a total of 328 calls were documented. Of these, 145 individuals commenced the survey, and 60.7% of them completed the questionnaire (n = 88). On the part of the senior physicians, 14.0% of the contacted senior physicians initiated the survey, with 10.3% completing the survey in its entirety. A response rate in the case of the survey of the architects cannot be specified for this survey since various associations were involved, and participants may have been members of multiple aforementioned associations. In the overall analysis, considering the existence of optional questions, a total sample size of 124 individuals emerged, comprising 36 senior physicians and 88 architects.
The selection of analysis variables was based on a meticulous evaluation of all available survey data. The objective was to identify variables that exhibited significant differences between the groups. Following a comprehensive review of the data, 14 out of 93 items were selected for their particularly distinct difference in response distributions between the groups. These questions were identified as meaningful identicators for relevant thematic areas and formed the basis for further statistical analysis. Initially, ten out of the 14 selected items exhibited a significant difference (s. Tables 2 and 3). After applying the Bonferroni correction, a significant difference remained in four out of the 93 items, which will be subject to further investigation ("rural environment", "division into pavillions", "visible cleanliness", "floor labeling").
Table 2 Listing of the 14 selected Items with their corresponding significance levelsTable 3 Ordinally scaled items that exhibited differences in the graphic-descriptive analysisRelevance of various factors in the selection of the clinic locationQuestion 3 of the ARCHI questionnaire examines the relevance of various factors in the selection of a clinic location. Four distinct factors are investigated in this context: connectivity to other clinical facilities, urban environment, rural environment, and accessibility via public transportation. The sample consisted of 36 senior physicians and between 84 and 88 architects, resulting in a total sample of 120–124 participants ("connectivity to other clinical facilities" n = 120; "rural environment" n = 121; "connectivity to public transportation" and "urban environment" n = 122).
For three of the four factors surveyed, there are no significant inter-group-differences, suggesting that both professional groups share a similar stance regarding connectivity to other clinical facilities, an urban environment and public transportation accessibility. More than two-thirds of respondents (82.5%; n = 99) would assert that connectivity to other clinical facilities is either “relevant” or “fully relevant”. Almost all respondents agree that connectivity to public transportation is “relevant” or “fully relevant” (95.1%; n = 116). Approximately half of the respondents (45.9%; n = 56) indicated that an urban environment should have no relevance in the choice of the clinic location.
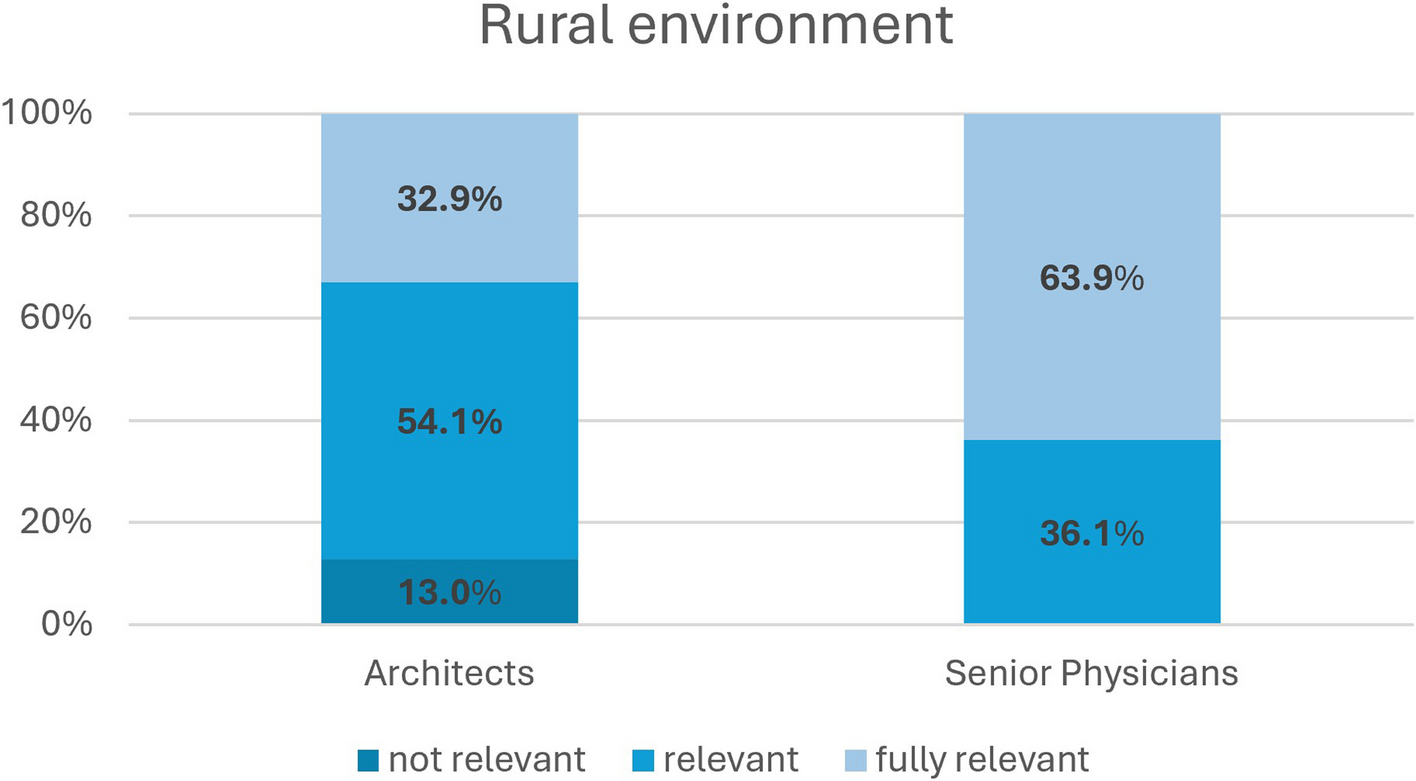
Regarding the significance of a natural and rural environment in the selection of the clinic location, there are divergent views between the two professional groups. Almost one-third of participating architects (32.9%; n = 28) would consider a rural environment to be “fully relevant” in the choice of hospital location, whereas none of the senior physicians rated a rural environment as “fully relevant” (s. Fig. 1). Conversely, over one-third of participating senior physicians (36.1%; n = 13) would say that the rural environment is “not relevant” in selecting a hospital, while only 12.9% of architects (n = 11) would express this view. In the quantitative analysis, the responses of the two professional groups were found to differ significantly (p < .001).
Fig. 1
Presentation of the distribution of the Likert scale for Question 3 (Rural environment)
Therapeutic benefits of different external architectural concepts in building structureThe ARCHI questionnaire assesses perspectives on the therapeutic benefits associated with various external building forms. The following external building forms are considered: "division of spaces into separate pavilions", "L-shape", "U-shape", "oval or elliptical shape", "E-shape", "star shape" and "atrium". The underlying dataset consisted of 36 responses from senior physicians and between 81 and 84 responses from architects, resulting in a total sample size ranging between 117 and 120 for different items ("atrium" and "L-shape" n = 120; "oval shape" n = 119; "star shape" and "E-shape" n = 118; "U-shape" n = 117).
Regarding the assessment of therapeutic relevance for building forms such as "atrium", "oval shape", "U-shape", "star shape", "L-shape" and "E-shape" no significant differences between professional groups were observed after applying the Bonferroni correction (see Table 2). The surveyed senior physicians and architects attribute the highest therapeutic benefit (82.5%) to the building form “atrium” and the lowest (47.5%) to the building form “E-shape” (see Fig. 2). In the evaluation of the therapeutic benefits of dividing spaces into separate pavilions, a significant difference between the two groups emerges.
Fig. 2
What therapeutic benefits do you attribute to the following external architectural concepts of the clinic’s building structure? Listed according to the highest therapeutic relevance (Atrium n = 120; oval shape n = 119; U-shape n = 117; starshape n = 118; L-shape n = 120; E-Shape n = 118)
A noteworthy majority of participating architects (53.7%; n = 44) assert that they perceive a “fully relevant” therapeutic benefit in a building structure with smaller units, such as pavilions, in contrast to a mere 8.3% (n = 3) of senior physicians who share this perspective. Over two-thirds of participating senior physicians (69.4%; n = 25) attribute no significant therapeutic benefit to the division of spaces into separate pavilions. The quantitative analysis reveals a noteworthy disparity in responses between the two professional cohorts, reaching statistical significance (p < .001).
Therapeutic relevance of decoration and interior designRegarding the relevance of various aspects in decoration and interior design, the ARCHI questionnaire examined four distinct factors: "flowers and plants", "visible cleanliness", "nature motifs as wall decoration", and "decoration created by patients in therapeutic everyday life". To address the research question, a total of 121 responses (36 senior physicians, 85 architects) were collected for the factors of "flowers and plants", "nature motifs as wall decoration", and "decoration created by patients in therapeutic everyday life", while 120 responses (36 senior physicians, 84 architects) were obtained for the factor of "visible cleanliness".
Concerning the first three factors mentioned, respondents are in agreement: Participants attribute the highest therapeutic relevance to the incorporation of decoration created by patients in therapeutic everyday life (90.9% fully relevant or relevant). Furthermore, more than four-fifths of respondents also perceive therapeutic in the factor of flower and plants (88.4% fully relevant or relevant). However, only slightly more than half of the respondents (55.4% fully relevant or relevant) ascribe therapeutic relevance to utilizing nature motifs as wall decoration in interior design. Regarding the factor of “visible cleanliness”, a significant difference between the surveyed groups is evident (see Table 2). In this context, more than four-fifths of all participating senior physicians (83.3%) would assert that visible cleanliness is “fully relevant”. Among architects, the therapeutic relevance is distributed as follows: 44.0% consider it “fully relevant”, 52.4% deem it”relevant”, and 3.6% deem it “not relevant”. In the quantitative analysis, a significant disparity in responses between the two professional groups is evident (p < .001).
Orientation in the building and on the wardDifferent systems can be employed for orientation within a medical facility, both on the ward and throughout the building. ARCHI introduces four distinct aspects for evaluation, providing respondents the opportunity to assess them: "floor markings", "general signage", "symbols and pictograms", and "colour coding". Data for the evaluation of "symbols and pictograms" and "colour coding" are available from 36 senior physicians and 85 architects (n = 121), "floor markings" from 36 senior physicians and 84 architects (n = 120) and "general signage" data from 36 senior physicians and 83 architects (n = 119).
Regarding "general signage", "symbols and pictograms", and "colour coding", there are no inter-group-differences, suggesting substantial agreement between the groups. Concerning the various means of orientation on the ward and in the building, respondents seem to perceive minimal differences, with the three aforementioned options appearing to be equally valued. However, in terms of providing orientation through floor markings (e.g., arrows), the two surveyed groups exhibit differences in their perspective.
In this regard, three-fifths of all senior physicians (61.1%; n = 22) stated that this was “not relevant”, contrasting with only 15.0% among architects (n = 13) who expressed the same view. The majority of architects (42.9%) find specific floor markings to be “fully relevant”. In contrast, only 2.8% of the senior physicians (n = 1) hold a similar perspective. The quantitative analysis reveals a significant disparity in responses between the two professional groups (p < .001).
Comments (0)