
Remember me
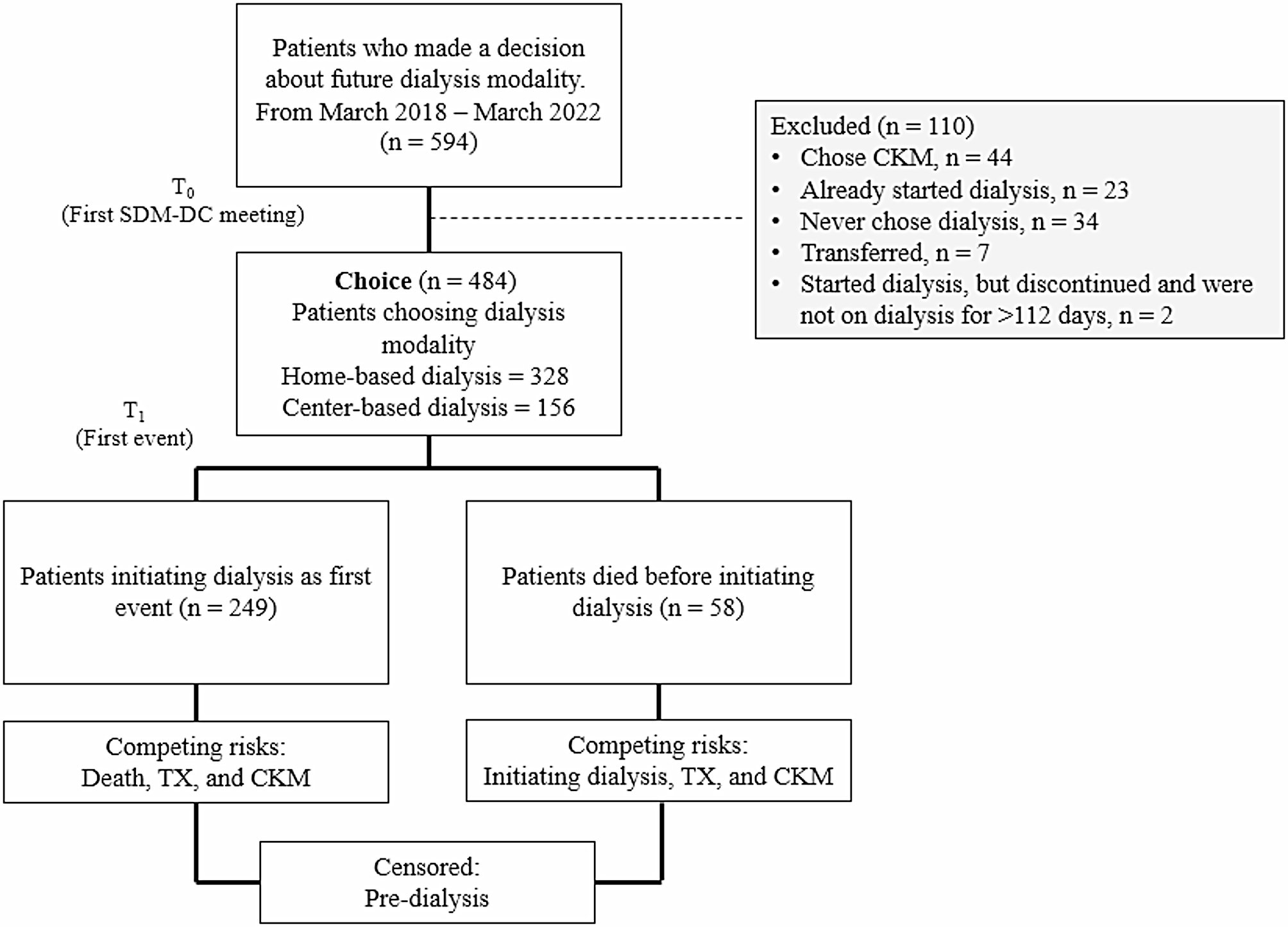






This study is the first to describe the pathway of patients with KF after an SDM-DC intervention.
The sample comprised 62% men, reflecting the proportion of men with kidney failure in Denmark [26]. Furthermore, 90% of the sample identified as ethnically Danish, aligning with the demographic composition of the general Danish population [27].
Home-based treatment was the preferred treatment for 68% of the participants. For patients’ progression to dialysis treatment, the results showed that half of the patients started treatment within 11 months of their first SDM-DC meeting. Furthermore, 83% initiated their initially chosen treatment, and predictor of interest for this was frailty. During the study, 12% of the patients died before initiating treatment. Both frailty and BMI were significant factors for this outcome.
Choice and outcomes for patients with KFWe did not observe significant differences in characteristics like ethnicity or number of SDM-DC meetings. However, due to the low proportion of non-ethnic Danish participants, we cannot conclude whether the intervention impacted social inequality. This underscores that patients received the necessary number of SDM-DC meetings to inform treatment choices effectively. Remarkably, our findings revealed a substantial preference for home-based dialysis (68%) in Denmark, notably higher than percentages reported in international studies (Pyart et al. 23%, Prieto-Valesco et al. 51%) [10, 11]. This divergence implies cultural and healthcare system influences on treatment decisions. The observed variations underscore the critical need for tailored interventions in kidney care, considering individual patient demographics and preferences. These insights not only contribute to the understanding of local and global trends but also advocate for healthcare strategies that align with the distinct needs of diverse patient populations. The study notes that the 11-month time frame for treatment initiation is not problematic, supported by findings showing no impact on changes in treatment choice over time. Notably, 83% concordance between chosen and initiated treatments exceeds international findings (56–77%), affirming the intervention’s effectiveness in maintaining treatment choices [12, 13, 28]. These insights suggest that the timing and concordance aspects of the intervention contribute positively to patient decision quality.
Outcome characteristics: Home-based dialysis, time, concordance, and deathAnalysing the characteristics of these outcomes, we surprisingly found that comorbidity was less of a predictor than frailty, and even with regard to death, frailty was a better predictor than comorbidity. This finding is consistent with those from Pyart et al. [10]. Although comorbidity and frailty represent related but distinct constructs, they capture different dimensions of patient health. CCI reflects disease burden based on objective diagnoses, while the CFS offers a broader and more holistic assessment that includes physical function, cognitive status, and social dependency. This may explain why frailty appeared more sensitive in predicting outcomes in our study. To date, frailty is only used in our setting for research and not as a clinical indicator. Few papers describe the use of frailty as a clinical indicator in nephrology, and these have not shown that using it as a clinical indicator yields improvement in the patient pathway [24, 29]. Our findings showed that frailty can predict which patients start dialysis in a time frame of 11 months, which experience less concordance between chosen option and initiated option, and which die before initiating dialysis. These findings suggest that using the frailty score in the decision-making process could support the patient in choosing the most suitable dialysis modality, but could also contribute to using the time from dialysis choice to initiation to improve their frailty in terms of nutritional status, performance status, and mental status [30]. Consistent with other studies [10, 21], a low BMI was a predictor for death before dialysis initiation. This finding identified a possible area for improvement in the patient pathway. Before initiating dialysis treatment, patients need an assessment of their nutritional status and, if they are at risk, can be recommended for referral to a dietician for nutritional intervention [31].
Not surprisingly a high eGFR predicted a longer time frame from dialysis choice to initiation. Some papers [32] suggest that dialysis choice should be at least six months before initiation to allow enough time to plan initiation properly. 50% of our patient population initiated dialysis within 11 months, and given the high concordance between chosen option and initiated option, we concluded that the referral criterion for the SDM intervention of an eGFR of less than 20 ml/min/1.73 m2 should not be changed – although the average eGFR was 13 ml/min/1.73 m2 (see Table 2). If we decrease the time-lag for the patient group waiting more than 11 months, we may possibly decrease the time frame for the patient group waiting less than 11 months.
One intervention, two hospitals, different outcomes, and different characteristicsThe results showed significant differences in the choice and concordance of treatment depending on whether the patient was affiliated with a regional hospital or a university hospital. More patients chose a home-based treatment at the university hospital compared to the regional hospital (see Table 2). The patient population at the university hospital live closer to the hospital, than the patient population at the regional hospital. In a US setting, travel distance and home dialysis rate have been established [33]. Furthermore, more patients achieved concordance at the regional hospital compared to the university hospital (see Fig. 3). No statistical significance was found between hospitals regarding time to dialysis initiation and death (see Figs. 2 and 4). The difference in concordance may be caused by the larger number at the university hospital choosing a home-based treatment, due to the fact the home-based treatment is the main predictor of not receiving the treatment chosen (see Table 2). The intervention itself is well defined but open to adaptation to each setting, suggesting that the difference should not be attributed to the intervention per se, but rather to how the intervention is delivered in practice and context. The literature emphasizes that one key barrier to the implementation of SDM is the engagement of healthcare professionals [34]. Healthcare professionals want what is best for the patient, but there is a lack of recognition that the patient’s values, opinions, and preferences are important and may potentially differ from professionals’ own [35, 36]. This can result in healthcare professionals recommending a decision that does not align with the patient’s preferences. Furthermore, healthcare professionals’ attitudes and skills are often considered to be crucial for successful SDM. Some healthcare professionals hold the view that they do not have the time, resources, or skills to engage in SDM [35, 36]. This highlights that there may be organizational and work culture differences between different hospital settings. Additionally, there may be differences in treatment focus or insufficient patient volume at a regional hospital for healthcare professionals to maintain their skills. Moreover, the results presented in Table 2 reveal that there was no difference in the number of SDM-DC meetings between the two hospitals. This underscores that the intervention was implemented in such a way that patients received the requisite number of SDM-DC meetings tailored to their needs. Disparities in treatment choices, therefore, must encompass more than merely the receipt of one or more SDM-DC meetings, highlighting that the differences are attributable to factors beyond the intervention itself. Rather, it could suggest the significance, for the patient, of comprehensive support from the entire interdisciplinary team. A previous study indicated that specific patients choosing a home-based treatment need support from the nephrologist, and the nephrologist must believe in the patient’s ability to cope with home-based treatment [37].
Fig. 3
Concordance between chosen and initiated treatment
Fig. 4
Time from first SDM-DC meeting to initiation of dialysis divided into over/under 11 months
LimitationsDue to the longitudinal design and retrospective follow-up resulting in an open and dynamic cohort, complete follow-up for all patients was not ensured. However, the statistical analysis method chosen facilitated inclusion of patients with varying follow-up times, taking competing events and censoring into account. Another limitation is that data were collected from EHRs and were not filed for the purpose of research, which may have caused misclassification of data. To ensure data validity, data from 10% of the patient population were checked by a clinician. On the other hand, collecting data from patients’ EHRs provided an opportunity to investigate a complete cohort with no dropout and ensured the findings represent patients and clinical practice as comprehensively as possible. At the university hospital, we chose to use eGFR as a momentary value. Data from the regional hospital were collected at a later date, and eGFR data were collected at baseline and one year before. eGFR slope was then calculated as a proxy for decline in kidney function. No associations were found between eGFR slope and the results, which is why we chose only to report the eGFR momentary value. In addition, data on albuminuria were collected but later excluded from the statistical analyses due to the risk of correlation between eGFR and albuminuria and the risk of type-1 errors. This study focused only on patients known to the nephrology clinic before dialysis initiation and does not cover the potential of the SDM intervention for patients with an acute start on dialysis. Furthermore, a notable limitation is the absence of data on patients who never chose a dialysis modality, representing 6% of those who received the intervention. Collecting relevant information on these patients could have helped identify distinguishing characteristics and enabled a comparison with the included cohort. Additionally, this study focused solely on baseline characteristics between home-based and center-based treatments, without performing a direct comparison of characteristics between the two hospitals. Such a comparison could have provided valuable insights into the factors underlying the observed differences in modality selection and concordance between the university and regional hospitals. Finally, generalizability of the study findings may be limited due to inclusion of only two hospitals and structural aspects of the Danish healthcare system, including its universal coverage and specific organization of nephrology care. The characteristics of the patient sample may also limit transferability to other contexts.
Comments (0)