This single-center retrospective cohort study was approved by the Institutional Review Board at Peking University People’s Hospital (approval number: 2024PHB384-001), and the need for written informed consent was waived.
The data analyzed in this study were retrieved from WiNEX, the Peking University People’s Hospital Integrated Electronic Medical Records System.
Participants and perioperative management
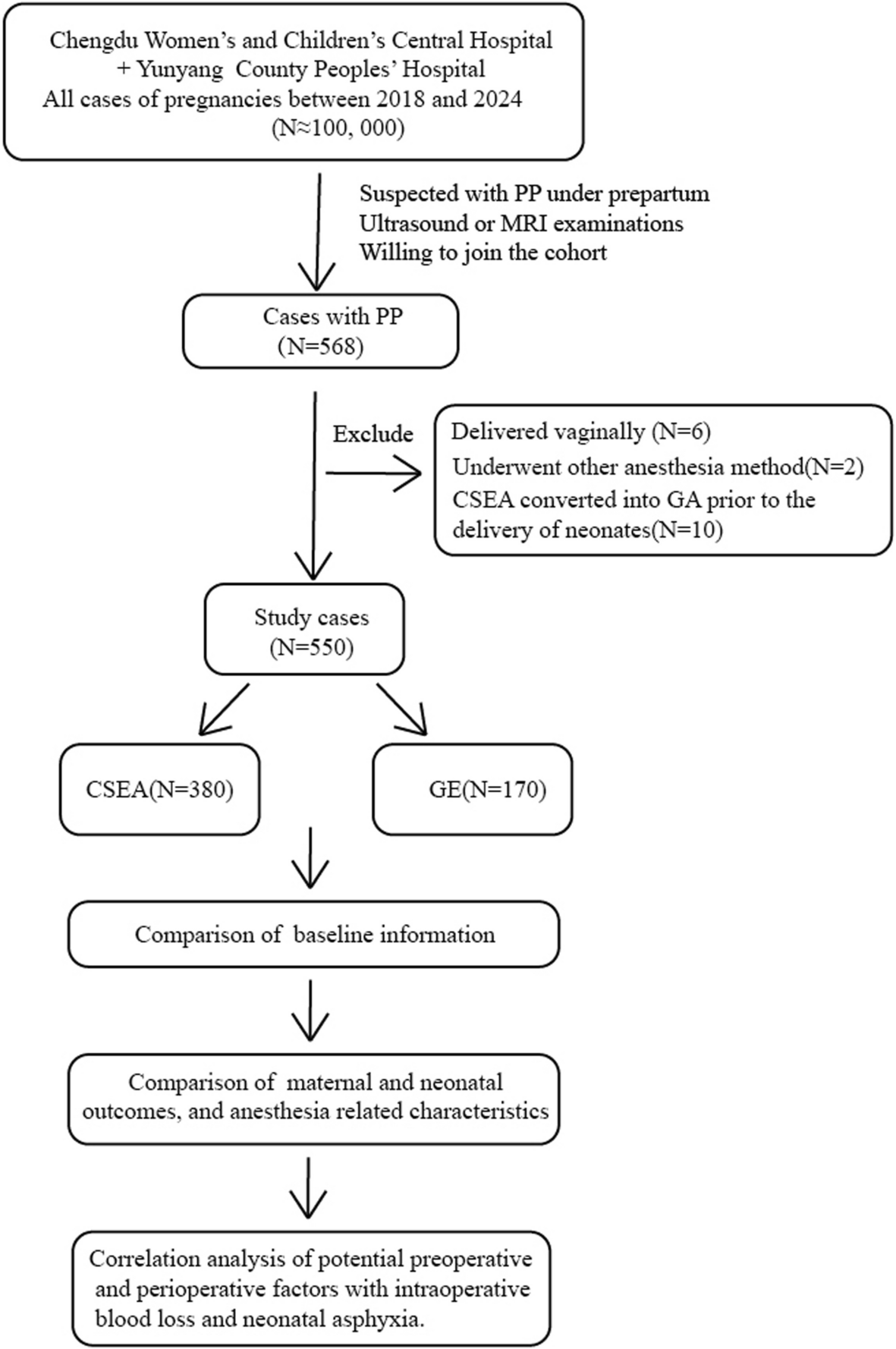
Patients aged 18–85 years who underwent thoracoscopic lung surgery at Peking University People’s Hospital between January 1, 2023, and October 30, 2024, were included. The inclusion criteria were as follows: (a) those received thoracic PVB (TPVB) for analgesia and (b) returned to the postoperative recovery room (PACU) after surgery. The exclusion criteria were as follows: (a) American Society of Anesthesiologists (ASA) physical status of patients greater than III; (b) bilateral TPVB; (c) bilateral thoracoscopic lung surgery or other concurrent types of surgeries; (d) those transferred to pneumonectomy; and (e) missing temperature data in the PACU.
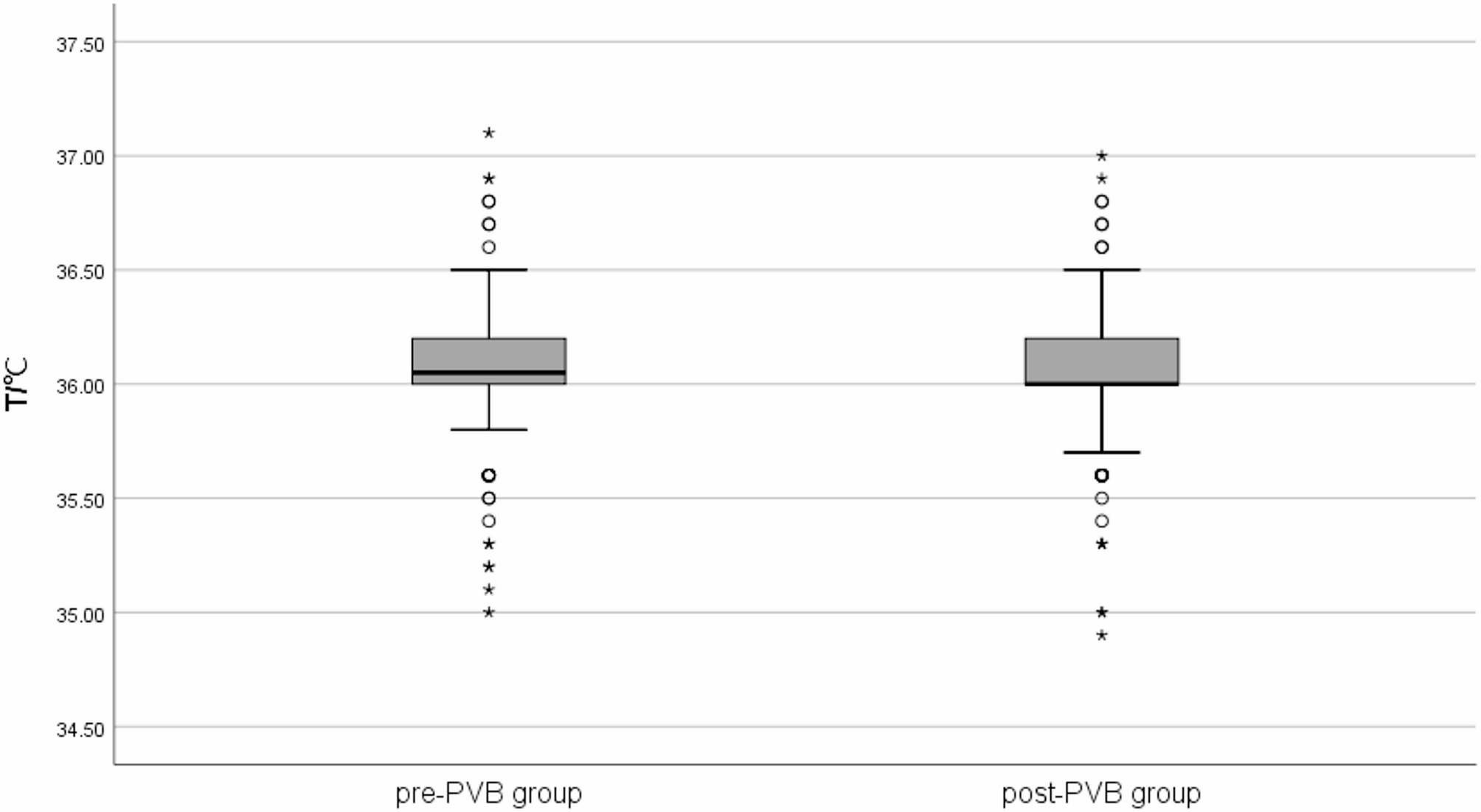
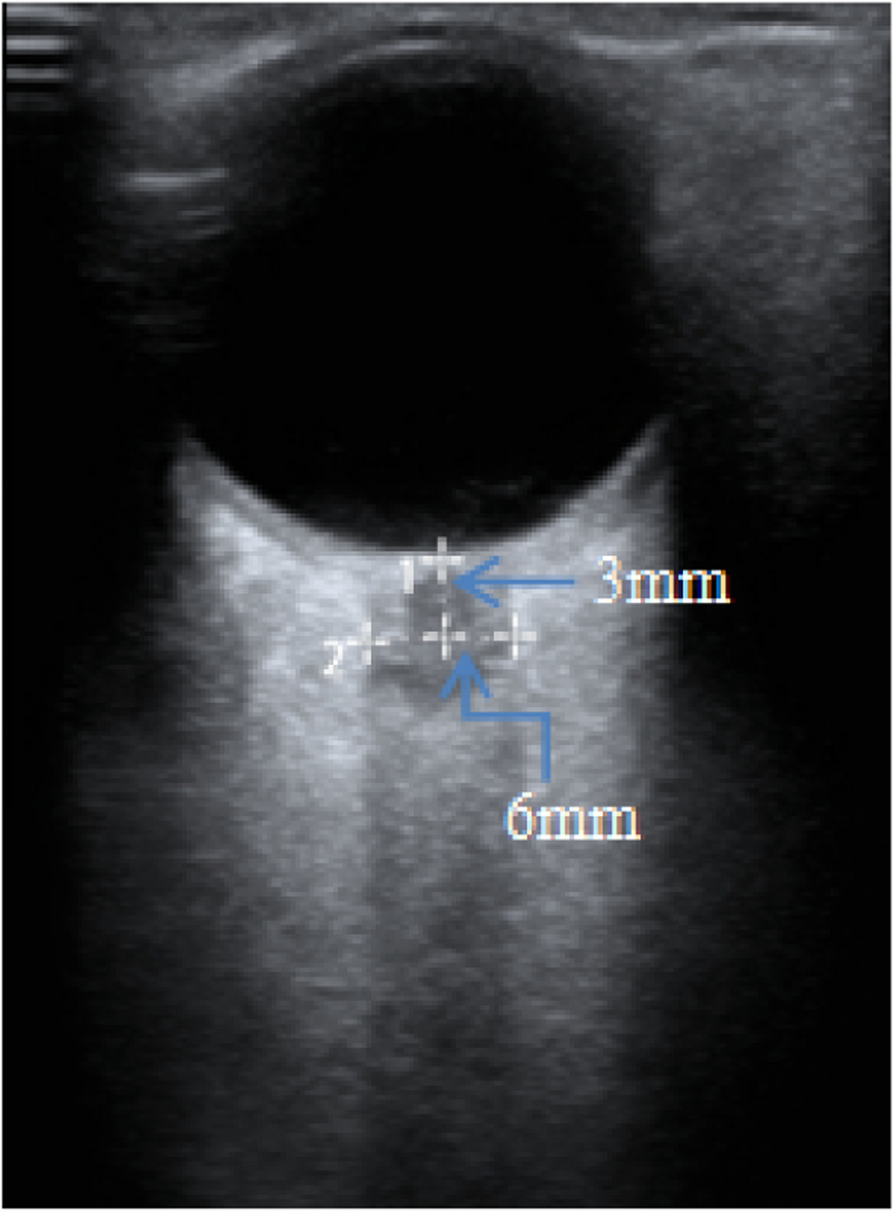
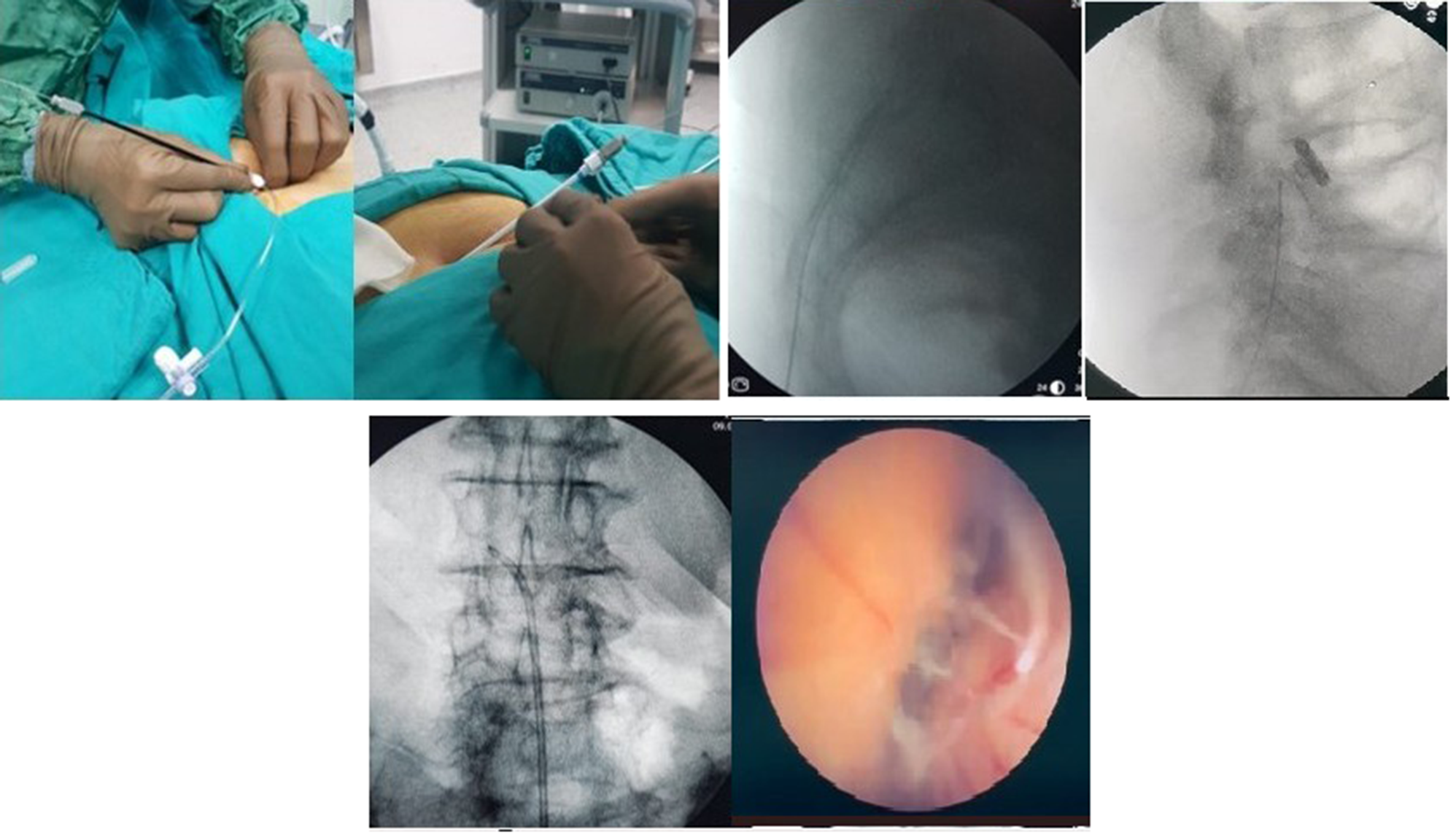
In our institution, the ambient temperature in the operating room and PACU is maintained at 22–25 °C. During surgery, active warming was routinely applied via a forced-air warming blanket. TPVB was performed by the anesthesiology team before the surgical incision or after closure of the skin incisions but before the patient emerged from general anesthesia. All the patients were divided into two groups: the preoperative PVB group (pre-PVB group) and the postoperative PVB group (post-PVB group). The TPVB procedure was standardized in both groups at the T3/T4 and T6/T7 thoracic paravertebral spaces via an out-of-plane technique guided by ultrasound, and 15 ml of 0.4% ropivacaine was administered to each space.
Data collection and outcome measures
The data collected included the following information: (a) basic characteristics, such as age, sex, height, weight, body mass index (BMI), ASA grade, and smoking history; (b) intraoperative interventions, such as the use of forced air-warming devices and heating infusion devices, inhalational anesthetics (sevoflurane or desflurane), dexmedetomidine and nonsteroid anti-inflammatory drugs (NSAIDs) (flurbiprofen axetil), opioid analgesics (sufentanil) and muscle relaxants (cisatracurium); (c) other intraoperative variables, such as operation type (wedge resection, lobectomy, segmentectomy, bullectomy, sleeve resection and others), baseline body temperature (the first nasopharyngeal temperature monitored during surgery), the lowest body temperature during the operation, the amount of intravenous fluid administered during surgery, estimated blood loss, blood transfusion volume, anesthesia and operation duration.
The primary outcome was the incidence of hypothermia according to the body temperature monitored in the PACU. In our study, hypothermia was defined as a nasopharyngeal temperature below 36 °C [3, 10]. The secondary outcomes were the occurrence of chill and delayed awakening, numeric rating scale (NRS) scores, extubation time (time from entering the PACU to extubation) and length of stay (LOS) in the PACU.
Statistical analysis
Continuous variables, such as age, height, weight, BMI, body temperature, transfusion volume, bleeding volume, dosage of opioid analgesics and muscle relaxants, anesthesia and operation duration, NRS score, extubation time and LOS in the PACU, are presented as the mean (standard deviation) or median [interquartile range] and were compared with independent samples t tests, Mann‒Whitney U tests or Wilcoxon rank sum tests. Categorical variables, such as sex, ASA physical status, smoking history, operation type, use of intraoperative forced air-warming devices and heating infusion devices, the administration of inhalational anesthetics, dexmedetomidine and NSAIDs, and the occurrence of chill and delayed awakening, were described as numbers (%) and were compared with Pearson’s χ2 test.
To reduce the effects of confounding factors, propensity score analysis was used to adjust for intergroup differences. All patient characteristics and perioperative parameters were used for adjustment. We subsequently used the derived propensity scores to match patients at a ratio of 1:1 via the nearest-neighbor matching method with a caliper of 0.2 for all patients to reduce the potential confounding effect of the covariates of baseline characteristics and surgical and anesthesia-related factors. The balance of variables before and after matching between the groups was assessed using standardised mean difference (SMD), with less than 0.10 indicating a balance [11].
Statistical analyses were performed via SPSS 26.0 (IBM Corp., Chicago, IL, USA). P < 0.05 was considered indicative of statistical significance.







Comments (0)