
Remember me






The retrospective study was approved by the Ethics Committee of Army Medical Center of PLA (No.10 ChangjiangZhilu, Yuzhong District, Chongqing 400,042, China) on February 7, 2024, Ethics Registration No was 2024-Research-14. The study complied with the ethical standards set out in the 1964 Declaration of Helsinki. An approval for exemption of patients from informed consent was obtained from the Ethics Committee of Army Medical Center of PLA. This study has been registered at https://www.chictr.org.cn/ (07/02/2024,ChiCTR MR-50–24–010856). Patients were included in the Group D, S and P, according to the intraoperative maintenance drug regimen. Inclusion criteria: 1) patients diagnosed with microangiopathy based on clinical symptoms, imaging, and laboratory tests; 2) those who have undergone microvascular decompression via retrosigmoid approach; 3) age 18–80 years old; 4) ASA I-III; 5) patients with complete clinical data, including complete examination and medical history. Exclusion criteria: 1) patients with concomitant ophthalmic diseases (ocular infection, glaucoma, cataract, blindness, etc.), history of ocular surgical trauma, and history of intraocular pressure increase; 2) those with a history of PONV and motion sickness; 3) patients who take anti-nausea and vomiting drugs or corticosteroids within 24 h before operation; 4) recent use of drugs that influence cerebrospinal fluid pressure, such as diuretics, glucocorticoids; 5) obesity (BMI ≥ 35 kg/m2); 6) difficult intubation; 7) patients coughing 3 min before each measurement time point; 8) peak intraoperative airway pressure > 30 cmH2O; 9) perioperative Neostigmine usage.
Anesthesia methodThe patients were fasted for 8 h and abstained from drinking for 2 h preoperatively, and when they entered the operating room. Arterial pressure (MAP), heart rate (HR), blood oxygen saturation (SpO2), electroencephalogram bifrequency index (BIS), body temperature (T), transcutaneous carbon dioxide monitoring (TcCO2) was measured prior to anaesthesia and after extubation of the tracheal catheter, and intraoperatively, end-expiratory carbon dioxide (EtCO2) was continuously monitored by the inbuilt sensors of anaesthesia machine, all of the above indices were measured and the values recorded.
Induction of anaesthesia: intravenous midazolam (0.03–0.05 mg/kg), sufentanil (0.3–0.5ug/kg), atracurium cis-benzenesulfonate (0.1–0.2 mg/kg), etomidate (0.1–0.4 mg/kg) were injected, and an airway tube was inserted through the mouth and connected to the anaesthesia machine for mechanical ventilation, oxygen mixture of 0.5 FiO2 and tidal volumes(VT) of 6–8 ml/kg, adjusted to maintain the end-tidal carbon dioxide partial pressure(EtCO2) between 30 and 45 mmHg.
Maintenance of anaesthesia: after tracheal intubation, BIS was maintained between 40–60 with different regimens. The following standardised protocol was used for the anaesthesia maintenance phase in all three groups: Group D: Dex 0.4ug/(kg.h) + Propo 4-12 mg/(kg.h) + remifentanil 0.1–0.2ug/(kg.min); Group S: 1–2% Sev + Propo 4-12 mg/(kg.h) + remifentanil 0.1–0.2ug/(kg.min); Group P: Propo 4-12 mg/(kg.h) + remifentanil 0.1–0.2ug/(kg.min). Surgery was performed with the patient in lateral decubitus position, posterior sigmoid sinus access, EtCO2:35–45 mmHg, body temperature maintained at 36–37 °C, and no positive end-expiratory pressure (PEEP). Sufentanil 10ug and tolansetron 5 mg were administered 30 min before the end of surgery; Sev and Dex were stopped 15 min before the end of surgery; Propo and remifentanil infusions were stopped at the end of surgery, the patient was returned to the flat position and transferred to the PACU.
Awakening and extubation: the patient was conscious and met the criteria for extubation, then the endotracheal tube was removed; the arterial blood gas analysis was measured 15 min after extubation and the patient was returned to the ward after reaching the Aldrete score = 10.
Management of complicationsTreatment of complications: Blood pressure was maintained within ± 20% of baseline MAP, and urapidil was used to lower blood pressure in the presence of hypertension; in the presence of hypotension (MAP < 60 mmHg), the infusion rate was accelerated and ephedrine 6 mg was infused intravenously, with norepinephrine pumped if necessary; in the presence of bradycardia (HR < 50 beats/minute), atropine 0.5 mg was infused intravenously. If agitation on awakening, administer 30–50 mg of intravenous propofol; if chills develop, apply heat from a warming fan to maintain body temperature; if the headache is mild and tolerable, place the patient on bed rest and administer oxygen; if the headache is intolerable and the VAS score is ≥ 3, administer tramadol intramuscularly or flurbiprofen ester intravenously, or oral loxoprofen sodium tablets once the patient is able to eat.VAS scores are based on calmness and absence of acute vomiting. VAS scores were performed when calm and without acute vomiting and were assessed every 4 h, with the highest VAS score recorded throughout the day. The nausea and vomiting grading methods selected was the 5-level classification method explicitly based on the frequency of vomiting in NCI-CTCAE v5.0 [9, 10]. Grading and management of PONV: Grade I: no nausea at rest, slight nausea during exercise, mild vomiting (1–2 times/d); Grade II: intermittent nausea at rest, moderate vomiting (3–5 times/d); Grade III: persistent nausea at rest, severe nausea during exercise, severe vomiting (more then 6 times/d). Grade IV: Life-threatening consequences, urgent intervention indicated; Grade V: Death. Grade II-V is classified as PONV. No treatment was needed when the patient presented with grade I vomiting; 10 mg of metoclopramide was given intravenously to treat the patient when he presented with grade II-V vomiting.
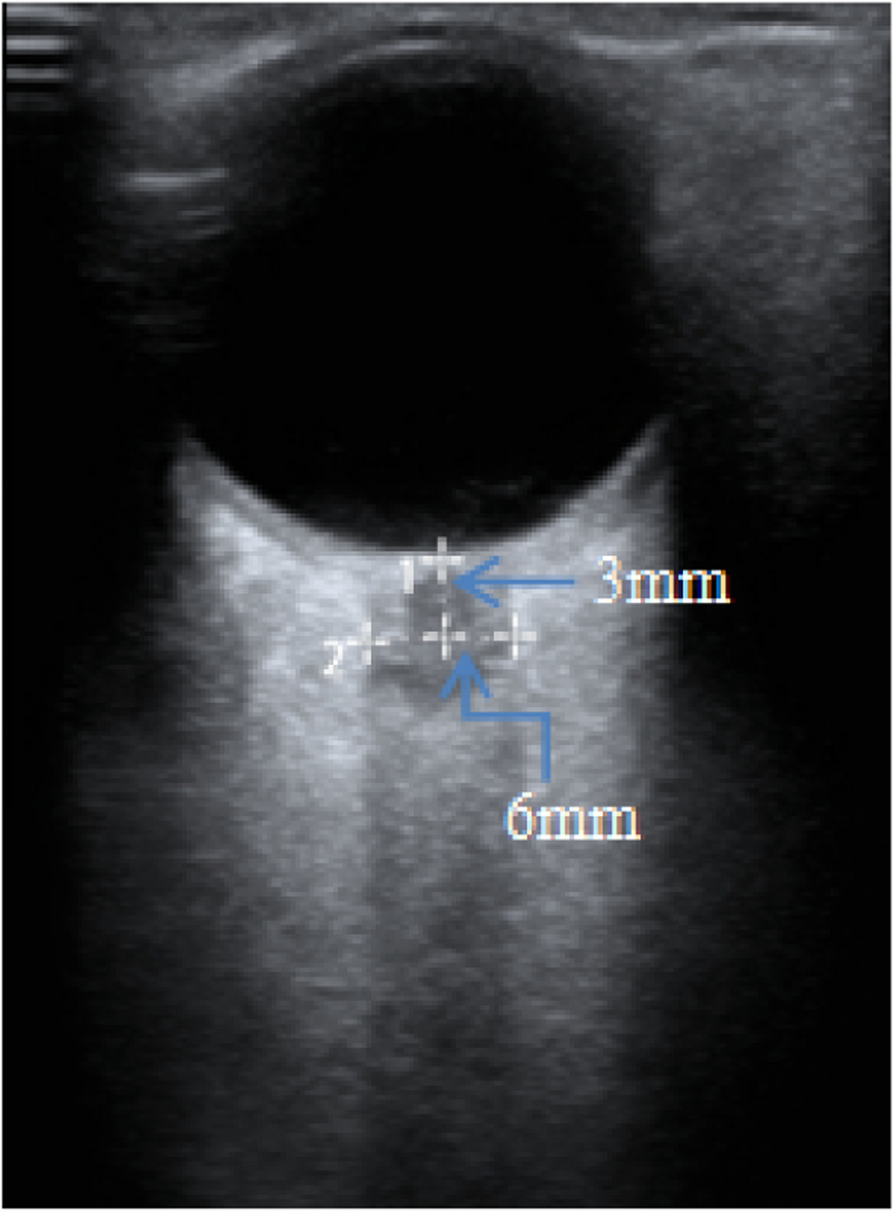
Measurement of ONSDONSD was assessed by the same anesthesiologist who measured the number of ONSD cases in more than 50 subjects guided by an ultrasonography specialist. The patient laid flat in the middle of the surgical table after entering the room. He shut the eyelids, both eyes were completely covered with 3M film, and the gel was applied on the surface of the film. The measurement depth was set to 4 cm, with the probe marking point facing to the right. The 7.5 mHz linear probe was gently placed on the eyelid. The probe was progressively moved from the frontal end to the nasal end to locate the optic nerve, and the search for the optimal transverse plane was completed by fine-tuning the probe. The ONSD was measured 3 mm posterior to the retina when the eyeball and optic nerve were visible throughout the ultrasound image. The probe was rotated 90 clockwise, when locating the longitudinal section of the optic nerve, with the probe marking point on the head side of the patient. The ONSD at each fixed time point was measured within 3 min, twice for each section, and eight times for sagittal and transverse sections, respectively. The average value of the eight measurements at each time point was recorded as the final value (Fig. 1).
Fig. 1
The ultrasonogram of optic nerve sheath. Note: Distance 1 is 3 mm posterior to the retina,distance 2 is the optic nerve sheath diameter,and the scale is in millimetres
Observation indicatorsMain observations: 7 time-point ONSD values (T0-T6), the number of occurrences of PONV and the use of drugs in different time periods. The seven time points are listed below, T0: 5 min before anaesthesia, T1: 10 min after tracheal intubation, T2: 10 min after lying on side in forward neck flexion, T3:at the end of the operation, T4: 10 min after return to horizontal position, T5: 10 min after removal of the endotracheal tube, and T6: on leaving the PACU. The three postoperative time periods are listed below, D0: 0–24 h postoperatively, D1: 24–48 h postoperatively, and D2: 48–72 h postoperatively.
Secondary observations: duration of anaesthesia, type and total amount of anaesthetic drugs used, patients’ postoperative VAS scores and use of analgesics.
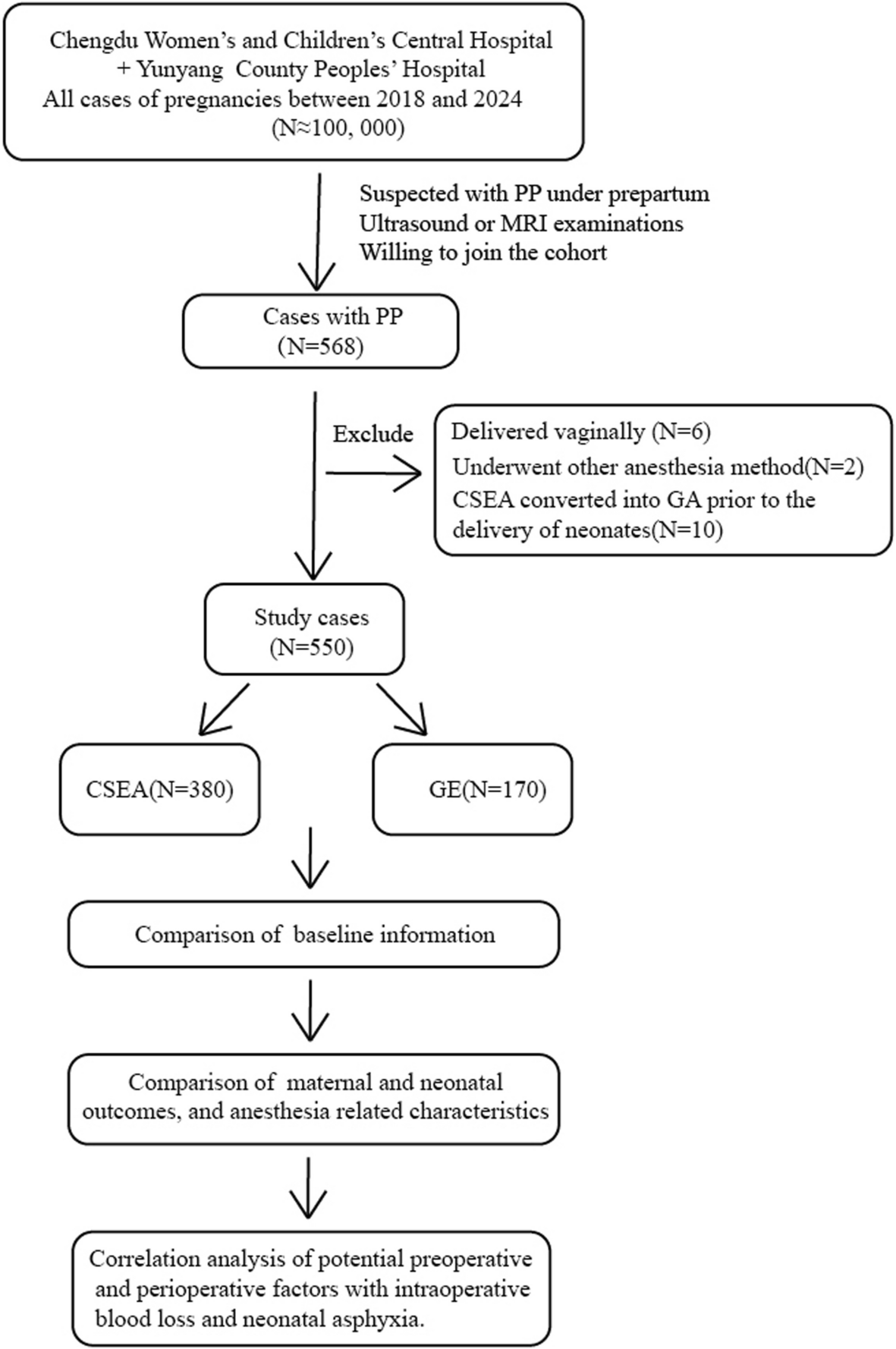
Statistical analysisThis study was a retrospective cohort analysis with data from the’Neurosurgical MVD Surgery Database of the Army Medical Center’from June 2023 to January 2024, and a total of 252 patients who underwent MVD were screened during the study period. Subgroups are based on actual anaesthetic medication maintenance programmes. A total of 135 patients were included according to the inclusion and exclusion criteria. After excluding 45 cases with missing data and inaccurate recording of ONSD and PONV measurements, 90 patients were finally included in the study for subsequent analyses and research work (Fig. 2).
Fig. 2
SPSS 26.0 software was used for statistical analysis. Continuous data, such as age, BMI, ONSD, etc., were tested for distribution using the Shapiro–Wilk test and expressed as mean ± standard deviation (x ± s) and independent samples t-test when they conformed to the normal distribution, and as median (quartiles) and Mann–Whitney U test when they did not conform to the normal distribution. Count data were expressed as N (%) using the C2 test or Fisher’s exact probability method. Repeated measures analysis of variance (ANOVA) was used for observations at different time points, and the Bonferroni method was used for post hoc multiple comparisons. Groups were classified according to the presence or absence of PONV, and variables with P < 0.05 were included in multifactorial logistic regression analyses with PONV as the dependent variable. The test level was α = 0.05 and P < 0.05 was considered statistically significant.
Comments (0)