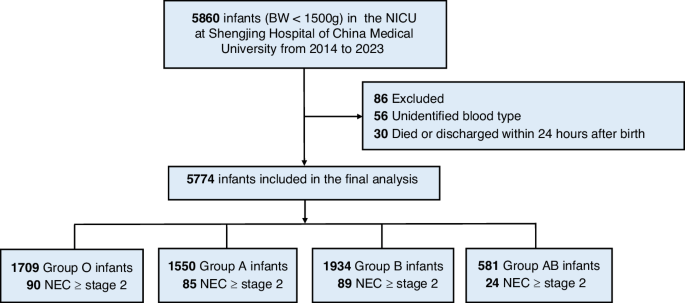
Since first proposed in 2012, blood group AB has been regarded as associated with an increased incidence and severity of NEC, as well as increased need for surgical intervention and mortality.7,20,21 However, this study, which included 5774 VLBW infants, did not find such associations. Compared to blood group O, there was no significant difference in the mortality and incidence of confirmed NEC (Bell’s stage ≥2) in blood group A, B, and AB. Furthermore, there were no differences in the incidence of severe NEC (Bell’s stage 3), need for surgery, or NEC-related death. Even when one blood group was compared with the other three combined, no differences were found. These results suggest that ABO blood group does not influence the incidence, severity, need for surgery, or mortality of NEC.
This discrepancy may stem from differences in cohort selection. Both the 20127 and 202120 studies analyzed cohorts of NEC patients and examined the distribution of ABO blood groups within these groups. The number of NEC cases in each blood group was influenced by the total population and the incidence of NEC in that group, which may have confounded the distributions of blood groups in their studies. In contrast, based on a large cohort of VLBW infants, we calculated and compared the ratio of primary outcomes in each blood group, expressed as the number of confirmed NEC cases in a blood group divided by the total number of VLBW infants in that group. This approach more accurately reflects the natural incidence of NEC in each blood group and ensures that subsequent statistical analyses are more reliable.
A 2021 study by Martynov et al.21 used a similar approach to ours. This multi-center study, which included 10,257 VLBW infants, concluded that blood group AB is a risk factor for surgical NEC, focal intestinal perforation, or death. Although these conditions share some clinical manifestations, focal intestinal perforation and NEC are distinct diseases, both predominantly affecting VLBW infants. Furthermore, 38.9% of the confirmed NEC cases in our study did not require surgical intervention, making Martynov et al.’s findings less comparable to ours, as our primary outcome included both confirmed NEC and mortality.
To minimize confounding factors, this study employed three multivariable models. The first model adjusted for infant and perinatal characteristics, including sex, GA, BW z-score, multiple gestation, antenatal corticosteroid use, premature rupture of membranes, chorioamnionitis, and asphyxia. The second model further accounted for maternal characteristics, while the third model incorporated the influence of admission year. Additionally, the impact of death or discharge against medical advice within 7 or 14 days after birth was also excluded (Tables S1–3). This stepwise approach yielded consistent results, indicating that ABO blood group does not independently influence the incidence or severity of NEC and mortality in VLBW infants.
In addition to statistical techniques, differing transfusion strategies may explain some of the discrepancies in findings. In our institution, leukocyte-depleted blood group-compatible RBCs are used for transfusions, whereas Thomson’s study7 utilized group O and Rh-negative RBCs for all recipients. Group O RBCs inevitably contain isoagglutinins, which may induce immune reactions, especially in recipients with blood group AB, who have antibodies against both type A and type B antigens. These immune reactions could potentially exacerbate the inflammatory cascade leading to NEC, although this hypothesis has not been experimentally validated. Transfusion with precisely matched RBCs might better eliminate the influence of isoagglutinins, providing a more “natural” epidemiological view of NEC.
ABO blood groups may influence NEC through interactions with the gut microbiota. Dysbiosis or aberrant production of microbiota metabolites has been implicated in NEC, and ABO blood group may affect the composition and growth of gut microbiota. Non-O blood groups (A, B, and AB) may secrete Fucosyltransferase 2, which serves as an adhesion receptor and energy source for Bacteroides and Faecalibacterium species in the gut.22 These bacteria help degrade complex plant polysaccharides into short-chain fatty acids like butyrate, which are crucial for maintaining intestinal barrier function.23 Bacteroides also plays a role in restoring bile acid metabolism and promoting the differentiation of regulatory T cells, thereby protecting against NEC.24 Moreover, Bifidobacteria, which are more abundant in the gut of non-O groups25, are known to protect against gut inflammation.26,27 Genes associated with ABO blood groups can regulate gut microbiota by influencing N-acetylglucosamine (GalNAc) levels.28 However, these findings are primarily based on experimental studies and have not yet been confirmed in clinical practice. Since the study population was VLBW infants, the effects of other factors such as gut immaturity, ischemia, and formula feeding may overwhelm the influence of ABO blood groups.
This study has several limitations. As a single-center study, the number of participants with blood group AB was relatively small, comprising only about 9–10% of the total population. This imbalance could introduce bias into the statistical analysis. However, the distribution of ABO blood groups in this study is quite similar to the natural distribution of the nearby provinces.29 Additionally, the influence of other factors, such as feeding protocols and antibiotic use, was not excluded from the analysis. Our explanations for the differences between our findings and those of previous studies are mostly hypothetical and should be further validated by future studies.


Comments (0)