
Remember me
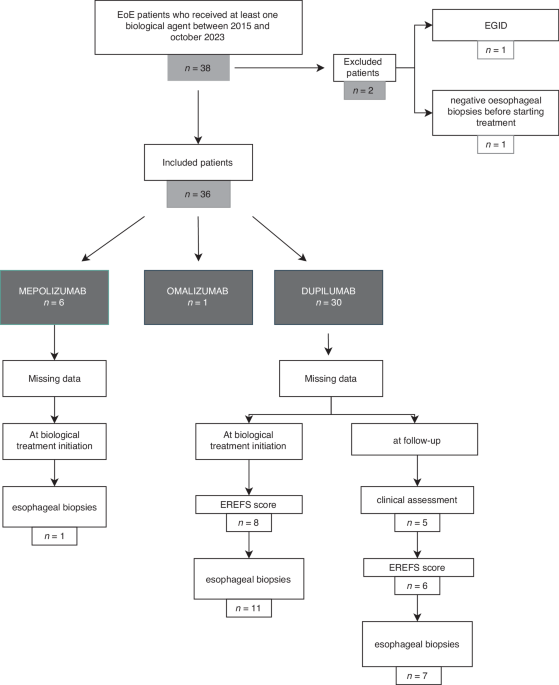

Thirty-eight patients from 14 tertiary care hospital centers were eligible for inclusion, with a median of 2 patients per center (min: 1, max: 7). Two patients were excluded because of an eosinophilic gastrointestinal disease and normal esophageal biopsies before initiating biological treatment (Fig. 1). Among the 36 included patients, 1 patient received two different biological agents (mepolizumab, then dupilumab). At follow-up, clinical data, EoE Endoscopic Reference Score (EREFS), and histologic data were available for 32, 31, and 30 patients treated with biological agents, respectively.
Fig. 1: Flowchart of the study population.
EGID eosinophilic gastrointestinal diseases.
At diagnosis, the mean patient age was 7.4 years, and most patients were male (75.0%, n = 27) (Table 1). Most patients presented with atopic disorders, including asthma (72.2%), FA (63.9%), AD (47.2%), or AR (38.9%). Five patients (13.9%) presented four atopic comorbidities, 11 patients (30.6%) had three atopic comorbidities, and 10 patients (27.8%) had two atopic comorbidities (5.6%). Only 3 patients reported no allergic comorbidities (8.3%). EoE symptoms were mainly dysphagia, food impaction, and feeding difficulties (Table 2). Endoscopic evaluation showed a median EREFS of 3.0 [interquartile range (IQR) 2.0; 4.0] and esophageal biopsies showed a median number of eosinophils/HPF of 23.3 [IQR 17.7; 32.7]. Most patients were prescribed proton pump inhibitors (PPIs, 97.2%, n = 35) for a median duration of 33.1 months, as well as budesonide (97.2%, n = 35) for a median duration of 14.7 months before initiating biologic therapy (Table 1). Almost half of the patients had empirical elimination diet (52.8%, n = 19) for a median duration of 4.9 months. In most cases, first-line treatments were initially combined (81.3%, n = 26/32 patients), with the most common combinations being PPI + budesonide (68.8%, n = 22/32), diet + PPI (25%, n = 8/32) and diet + budesonide (15.6%, n = 5/32)(Supplementary Table). Failure of first-line treatments was the main real-life reason for starting biological therapy (75.7%, n = 28). In the absence of authorization in France for EoE, the main reason declared for prescribing biologics was compassionate use (54.1% n = 20) pending a recommendation in EoE in France. The average time from EoE diagnosis to commencement of biologic therapy was 47.8 months ( ± 26.9). Symptoms and endoscopic findings present before starting the biological agent are detailed in Table 1.
Table 1 Characteristics of the study population at the time of initiation of biological therapy.Table 2 Comparison of the study population with children receiving conventional therapies from the 2 European registers.Biological agents and follow-upOmalizumabOne patient (male, 11 years) received omalizumab starting in February 2022 to treat severe asthma, at a dosage of 600 mg every 14 days. Heartburn was reduced from once or twice a day to once a month, after treatment. This patient did not present any other symptoms associated with EoE. However, after 16 months of omalizumab, although the number of asthma exacerbations was reduced, worsening of the obstructive ventilatory disorder led to switching to treatment with dupilumab. Endoscopic assessment was performed 9.6 months after starting treatment. EREFS was 2 and 0 before and after treatment, respectively. Complete histological remission was observed (0, 51, and 27 eosinophils/HPF before and 0, 0, and 1 eosinophils/HPF after omalizumab, in the proximal, mid-, and distal esophagus, respectively). The patient did not report any side effects while receiving omalizumab. Treatment with dupilumab was not included in the study because of complete remission prior to initiation.
MepolizumabMepolizumab was prescribed to 6 patients at the doses recommended for severe asthma, i.e., 40 mg monthly for patients aged 6–11 years (n = 2) and 100 mg weekly for patients older than 12 years (n = 4). Clinical efficacy was partial after 6–12 treatment months (Fig. 2a). The mean time to endoscopic control was 6.9 months. Histological response was absent in 3 patients, complete in 2, and partial in 1. EREFS was similar before and after treatment (median score 2.5 both before and after mepolizumab). Mean eosinophil counts were 35, 37, and 18 eosinophils/HPF before and 6, 9.5, and 4 eosinophils/HPF after mepolizumab, in the proximal, mid-, and distal esophagus, respectively (Fig. 2b). No side effects were reported. Two patients were still treated with mepolizumab at the time of data collection. Mepolizumab was suspended for complete remission in 3 patients and for treatment non-adherence in 1 patient.
Fig. 2: Effects of mepolizumab on EoE.
a Clinical symptoms, before and 6-12 months after initiating mepolizumab. b Eosinophils count per HPF at the proximal, mid- and distal esophagus. EoE eosinophilic esophagitis, HPF high power field.
DupilumabThirty included patients received dupilumab, among whom 12 were followed prospectively. Eleven patients received dupilumab at recommended doses for severe AD: 5 patients were prescribed 200 mg/2 weeks; 6 patients were prescribed 300 mg/2 weeks. Dupilumab was also prescribed at recommended doses for severe asthma in 5 patients: 200 mg/4 weeks in 3 patients and 300 mg/4 weeks in 2 patients. For 4 patients (13.3%), dupilumab was administrated weekly (300 mg for 3 patients and 200 mg for 1 patient). Most patients (76.6%, n = 23) started dupilumab due to previous treatment failure. Compassionate use was indicated, in accordance with marketing authorization, for half (n = 15) of these patients, while severe asthma (26.7%, n = 8) and severe AD (16.7%, n = 5) were the second and third indications.
In terms of overall clinical efficacy, all patients’ symptoms improved after 6–12 months of dupilumab (Fig. 3a). Clinical improvement was significant (p = 0.0009), with complete resolution of symptoms in almost half of patients (48.0%, n = 12). Among these twelve patients, 6 (50%) were treated 300 mg every 2 weeks, 5 (41.7%) had 200 mg every two weeks and one (8.3%) received 200 mg monthly. Substantial improvement of food impaction (p = 0.01) and dysphagia (p = 0.0005) were observed on treatment.
Fig. 3: Effects of dupilumab on EoE.
a Clinical symptoms, before and 6-12 months after initiating dupilumab, food impaction: p = 0.011; dysphagia: p = 0.0005. b Eosinophils count per HPF at the proximal, mid- and distal esophagus, *p = 0.001, **p = 0.0001, ***p < 0.0001. EoE eosinophilic esophagitis, EREFS edema, rings, exudates, furrows, stenosis, HPF high power field.
Endoscopic control was performed at 7 months (mean 7.0 ± 4.5) and revealed a complete histological response for most patients (82.6%, n = 19), but was partial (8.7%, n = 2) or absent (8.7%, n = 2) for the others. Patients showing complete histological remission, mostly received 300 mg every 2 weeks (42.1%, n = 8) and 200 mg every 2 weeks (31.6%, n = 6). The median EREFS significantly decreased (3.0 vs. 0, p < 0.0001). For each esophageal stage, significant reduction of eosinophil counts before and after dupilumab are detailed in Fig. 3b.
Side effects were assessed in 26 patients and revealed good tolerance of dupilumab by most, who reported no adverse effect (76.9%, n = 20). Several patients reported pain at the injection site (11.5%, n = 3). One patient had blepharitis (3.8%) 3 months after starting dupilumab. One patient experienced a combination of abdominal pain, rash, and fever after the first injection, without the need to discontinue treatment. One patient (3.8%) experienced asthenia in the days following each injection. Side effects were not assessed in 4 patients because treatment had been started since less than 6 months. Dupilumab was still ongoing at the time of data collection for 25 patients (83.3%). Treatment was discontinued for 5 patients, due to complete remission for 3 patients, poor compliance for 1, and side effects for 2 (blepharitis in 1 patient who had severe active AD at the start of treatment).
Comparisons with pediatric patients with EoE from European Registries, treated with conventional therapiesWe compared our cohort with pediatric patients, who were naïve to biologics, from the two European registers pEEr (n = 582)18 and EoE CONNECT (n = 254)19 (Table 2). Though age was not analyzed statistically, patients who required biologics in our cohort appeared younger at diagnosis (mean age 7.4 vs. 11.9 years). Patients did not differ on sex or AR frequency. However, our patients displayed significantly more FA, asthma, and AD compared with pEEr- and EoE CONNECT-registered patients. Our patients reported more symptoms than those on conventional therapies, including dysphagia, food impaction, vomiting, regurgitations, abdominal pain, and failure to thrive (Table 2). Finally, patients requiring biologics presented more exudates (p = 0.01), furrows (p = 0.0003), and a more frequent fibrostenotic phenotype (p = 0.0007) at baseline.
Comments (0)