
Remember me







The KNHANES is a nationwide population-based cross-sectional survey conducted by the Korea Disease Control and Prevention Agency. The survey employs a stratified, multistage cluster sampling design to ensure that the sample is representative of the Korean population. KNHANES collects comprehensive health, nutrition, and lifestyle data through standardized health interviews, physical examinations, and laboratory tests [21].
For this study, we utilized KNHANES data collected from 2019 to 2021. Trained specialists conducted ophthalmic examinations using standardized protocols to assess visual fields, IOP, and optic nerve structure. Visual field tests adhered to reliability criteria, including fixation error ≤ 1 and false-positive rates ≤ 1%. The paper by Song and colleagues describe the methodological details of KNHANES [22].
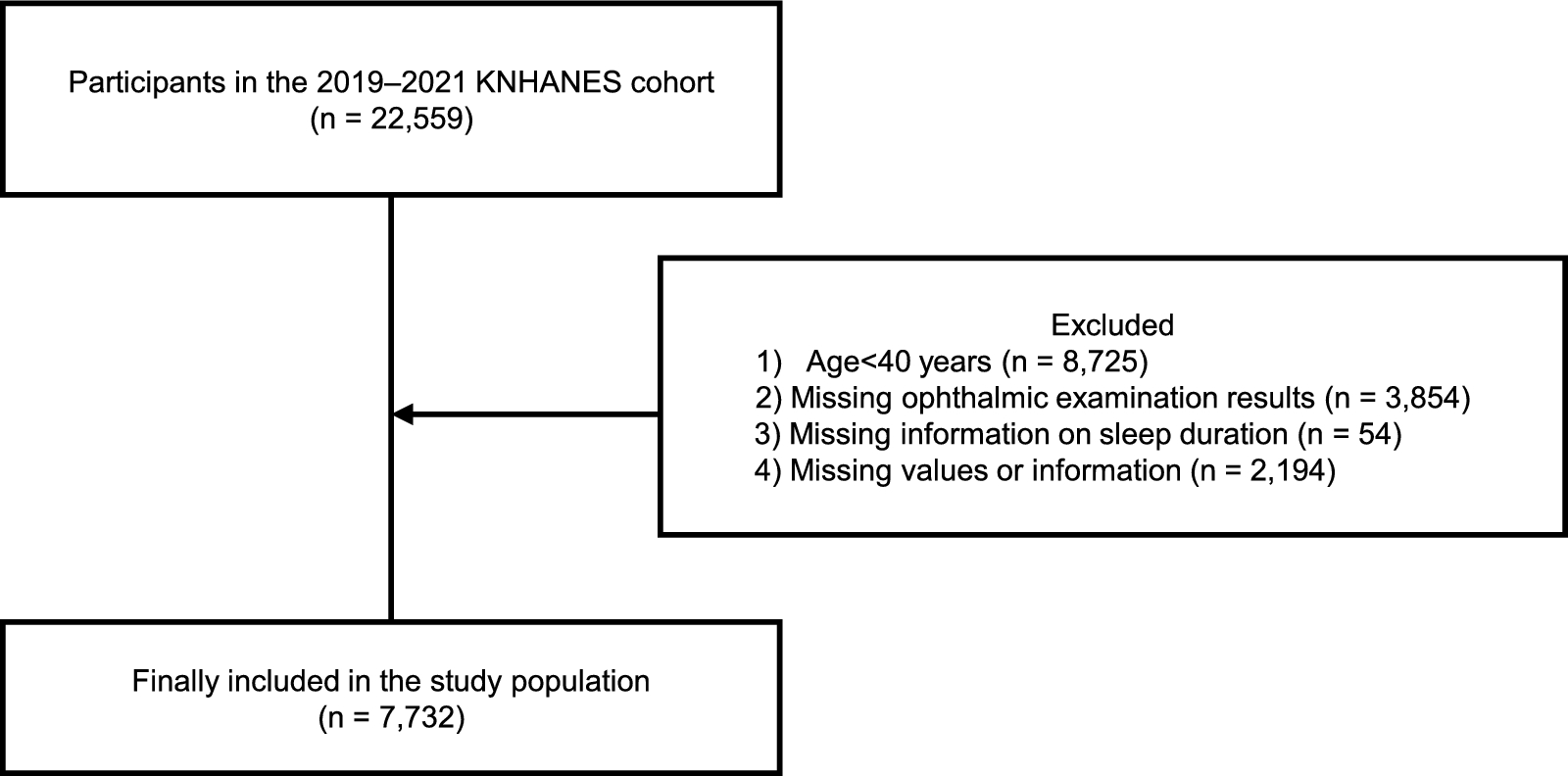
Study populationOf the 22,559 participants surveyed between 2019 and 2021, 7,732 were included in the final analysis after applying the following exclusion criteria: (1) individuals < 40 years old (n = 8,725), (2) those without ophthalmic examination data (n = 3,854), (3) those lacking sleep duration data (n = 54), and (4) those with missing values for key variables (n = 2,194). The final sample consisted of participants aged ≥ 40 years with complete ophthalmic and sleep-related data, allowing us to investigate the relationship among OSA risk, sleep duration, glaucoma prevalence, and IOP. The process of selecting the study population is summarized in Fig. 1.
Fig. 1
Selection of the study population
This study adhered to the guidelines of the Declaration of Helsinki. Institutional Review Board (IRB) approval was obtained from the Samsung Medical Center (IRB No. SMC 2024–08-090; IRB examination exemption approval). The IRB waived the requirement for individual informed consent because of the retrospective design and use of publicly available data. Informed consent was obtained from all participants prior to their enrollment in the KNHANES, in accordance with the ethical guidelines.
MeasurementsSmoking was defined as an adult who had smoked more than five packets of cigarettes (100 cigarettes) during their lifetime. Drinking was defined as drinking alcoholic beverages at least once a month during the past year. Individuals who graduated from high school were classified as having a high level of education. The regions were allocated into two groups: urban (Seoul, Ulsan, Daejeon, Incheon, Busan, Daegu, Gwangju, Sejong, and Gyeonggi) and rural (the rest). Low-income households were categorized as those belonging to the lowest quartile. High physical activity was defined as ≥ 10 metabolic equivalent task (MET)-h/week which is the amount of physical activity recommended by the World Health Organization (WHO) [23]. The MET measures energy expenditure and was calculated using the Global Physical Activity Questionnaire [23]. Stress was defined when responses are “very high” or “high” to the question “What is your stress level in your daily life?”. Body mass index (BMI) was calculated as weight (kg)/height2 (m2). Waist circumference (cm) was measured at the midlevel between the highest and lowest iliac crests. Neck circumference (cm) was measured in the seated position. Individuals receiving glaucoma treatment were categorized as ‘glaucoma treatment’, whereas others were categorized as ‘no glaucoma treatment’.
Systolic (SBP) and diastolic blood pressure (DBP) were taken as the average values of the second and third trial among three trials. Blood pressure was measured after a minimum of 5 min of rest in a seated position. Hypertension was defined as taking antihypertensive medication, SBP ≥ 140 mmHg, or DBP ≥ 90 mmHg. Total cholesterol, high-density lipoprotein (HDL), fasting plasma glucose (FPG), triglycerides (TG), and glycated hemoglobin (HbA1c) concentrations were measured in blood samples obtained after 8 h of fasting. According to the modified NCEP-ATP III criteria [24], a metabolic syndrome diagnosis was made when an individual met three out of the following five criteria: (1) waist circumference ≥ 90 cm for men and ≥ 80 cm for women, (2) serum TG concentration ≥ 150 mg/dL, (3) serum HDL concentration < 40 mg/dL for men and < 50 mg/dL for women, (4) taking antihypertensive medication or SBP ≥ 130 mmHg or DBP ≥ 85 mmHg, or (5) FPG concentration ≥ 100 mg/dL or undergoing diabetes treatment. Hypertriglyceridemia was defined as TG ≥ 200 mg/dL. Diabetes was defined as a fasting glucose level ≥ 126 mg/dL, HbA1c ≥ 6.5%, current use of oral hypoglycemic agents or insulin injections, or a previous diagnosis of diabetes.
The ophthalmic examinations included visual field tests, IOP measurements, and optical coherence tomography (OCT). Ophthalmic examinations were performed for participants aged 40 years or older in the 2019–2020 survey, and for those who were 19–59 years old in the 2021 survey [22]. The IOP was measured six times, with the final value defined as the average of the six measurements. IOP was measured for both eyes, and the average IOP of both eyes was used for analysis. Refractive error was defined as a mean refractive error of both eyes. Further details of the KNHANES are available in a previously published paper [22].
Definition of STOP-BANGThe components of STOP-BANG (snoring, tiredness, observed, pressure, BMI, age, neck circumference, gender) were defined as follows [11].
“Snoring”, “tiredness”, and “observed” were defined as a response of “Yes” to the following questions, respectively: “Do you snore loud enough to be heard through closed doors or louder than your voice?”, “Do you often feel tired, fatigued, or sleepful during the daytime?”, and “Did anyone notice if you stopped breathing while you were asleep?”. “Pressure” was defined as an SBP ≥ 140 mmHg or a DBP ≥ 90 mmHg or on antihypertensive medication and “BMI” as those with a BMI > 30 kg/m2, modified according to the WHO guidelines for severe obesity in Asians [25]. “Age” was defined as 50 years old or older, “neck” as in neck circumference ≥ 40 cm [11], and “gender” as male.
Participants with a score of 3 or higher on any of the abovementioned eight items were categorized as having a high risk of OSA, and those with a score of 2 or lower as having a low risk of OSA [11].
Definition of sleep durationSleep duration was assessed using a questionnaire. For participants in the 2019–2020 cohort, the question “How long do you usually sleep per day?” was answered in hours (h) for each weekday (working days) and weekend (nonworking days or the day before nonworking days). For participants in the 2021 cohort, the question “When do you usually go to bed and when do you usually wake up?” was answered to the nearest minute on weekdays and weekends. While weekday and weekend sleep durations were obtained from the data, the overall weekday sleep duration was calculated as (5 × weekday sleep duration + 2 × weekend sleep duration)/7.
Abnormal sleep duration was defined as < 7 h or > 9 h, consistent with prior studies linking insufficient and excessive sleep to adverse health outcomes [26, 27]. To examine how sleep duration modifies the relationship between OSA risk and glaucoma or IOP, we performed interaction analyses using specific cutoffs (< 9 h for glaucoma and < 8 h for IOP) identified from observed data patterns.
Definition of glaucomaGlaucoma was diagnosed according to the guidelines of the International Society of Geographical and Epidemiological Ophthalmology [28], as the presence of glaucomatous visual field defects with glaucomatous structural changes. Absence of fixation errors and a false-positive error ≤ 1, along with at least one location of reduced sensitivity corresponding to an optic disc or retinal nerve fiber layer abnormality, was defined as a glaucomatous visual field defect. Glaucomatous structural change was defined as the presence of at least one of the following: vertical cup-to-disc ratio ≥ 0.7, neuroretinal rim thinning or notching, a retinal nerve fiber layer defect, or an asymmetrical cup-to-disc ratio ≥ 0.3. When a reliable visual field test result was unavailable, glaucoma was defined by the presence of at least one glaucomatous structural change: thinning or notching of the neuroretinal rim with a cup-to-disc ratio ≥ 0.9, a corresponding retinal nerve fiber layer defect, or an asymmetrical cup-to-disc ratio ≥ 0.3. In the absence of both visual field test results and fundus images, glaucoma was diagnosed by a corrected visual acuity ≤ 10/200 and an IOP exceeding the 97.5th percentile.
Statistical analysisAll statistical analyses were conducted using R (version 4.3.1; R Foundation for Statistical Computing, Vienna, Austria). The normality of continuous variables was assessed using histograms. Age, refractive error, neck circumference, fasting blood glucose levels, and sleep durations were not normally distributed. Continuous variables are presented as means ± standard error (SE) for consistency across variables and to facilitate interpretation and comparison with previous studies. Categorical variables are presented as proportions (% ± SE).
Multiple logistic regression models for complex survey sampling were applied to examine the association between glaucoma prevalence and the components of the STOP-BANG questionnaire, OSA risk levels, and abnormal sleep duration across different periods (overall week, weekdays, and weekends). These models were adjusted in sequential stages as follows: Model 1 was unadjusted; Model 2 was adjusted for gender and age; Model 3 was additionally adjusted for smoking, drinking, physical activity, education level, and income level; and Model 4 was adjusted for IOP, metabolic syndrome, stress level, and refractive error. For subgroup analysis, the association between OSA risk and glaucoma prevalence was examined within each sleep duration category (< 6 h, 6 h ~ < 7 h, 7 h ~ < 8 h, 8 h ~ < 9 h, and ≥ 9 h) for overall week, weekday, and weekend durations. Interaction terms were included to assess the effect of sleep duration modification (< 9 h vs. ≥ 9 h) on the relationship between OSA risk and glaucoma prevalence.
The relationship between IOP and the components of the STOP-BANG questionnaire, OSA risk, and abnormal sleep duration across the same time periods were assessed using multiple linear regression for complex sampling. Associations between OSA risk and IOP were further evaluated within each sleep duration subgroup (< 6 h, 6 h ~ < 7 h, 7 h ~ < 8 h, 8 h ~ < 9 h, and ≥ 9 h) across the overall week, weekday, and weekend periods using Student’s t-test, and interaction terms were included in the linear regression models to investigate the interaction between sleep duration (< 8 h vs. ≥ 8 h) and OSA risk for effects on IOP. Adjustments were applied in the same sequence across the models as described above, except for Model 4, which excluded the IOP to avoid repetition and included glaucoma treatment. In models that analyzed individual components of the STOP-BANG questionnaire, age and gender variables were excluded for the respective STOP-BANG components “age” (≥ 50 years) and “gender” (male) to avoid redundancy.
All statistical tests were two-sided, with a P value of less than 0.05 indicating statistical significance.
Comments (0)