The current study provides valuable insights into the epidemiology, diagnosis, and management of rectal NETs in India. To the best of our knowledge, this is the first study evaluating this disease subset in this geography.
Our patients presented at a slightly younger age with a median age of 50 years compared to the global median of 56–57 years. We also had a slight male preponderance, and the foci was more often in the low rectum compared to published literature where mid-rectal disease predominates. While these could be related to the small sample size of our cohort or the referral bias, this report identified some other key differences of the disease in our region compared to the world. Patients presented with both clinically advanced disease and a more aggressive tumour biology compared to those observed in other regions. Contrasting with Western data, our patients presented with larger tumour sizes (37 mm) compared with a global median of 10–20 mm, more advanced stages (81% presented with T2 + disease compared with less than 20% globally), and poorer disease grades (82% had Grade II/III disease compared with 80–90% having Grade I globally) [12,13,14].
For Grade I disease, the lesion sizes observed aligned with global data. However, the predominance of higher-grade lesions likely contributes to the overall larger median tumour size observed. While late presentation, non-specific symptoms, and a lack of screening colonoscopy may explain the larger tumour sizes and advanced AJCC stages, it is crucial to note that many of our patients had higher-grade tumours, elevated MIB/Ki-67 indices, and increased serum CgA levels—all markers of recurrence risk and aggressive tumour biology [15]. This pathological aggressiveness contrasts with findings from studies in China [16], South Korea [17], and Japan [18], suggesting potential biological differences in the disease affecting patients in the Indian subcontinent.
Recent research has also suggested the possible role of insulin resistance, metabolic syndrome, and lipid dysregulation, which can be contributory to development of many cancers including NETs [19]. While these risk factors are common in our cohort, data to differentiate correlative vs causative relationship in Indian patients is not available. Reports also suggest that our population may have the CpG island methylator phenotype [20, 21], which could contribute to the poorer outcomes in our cohort.
Globally, rectal NETs present early and when concern for recurrence is low, organ sparing and quality of life decisions take centre stage. As a result, most guidelines recommend endoscopic management in management of localised rectal NETs [22, 23]. While modified endoscopic mucosal resection (mEMR) is equivalent to endoscopic submucosal dissection (ESD) in < 10 mm lesion size, ESD is preferred for > 10 mm lesions and in the salvage setting.
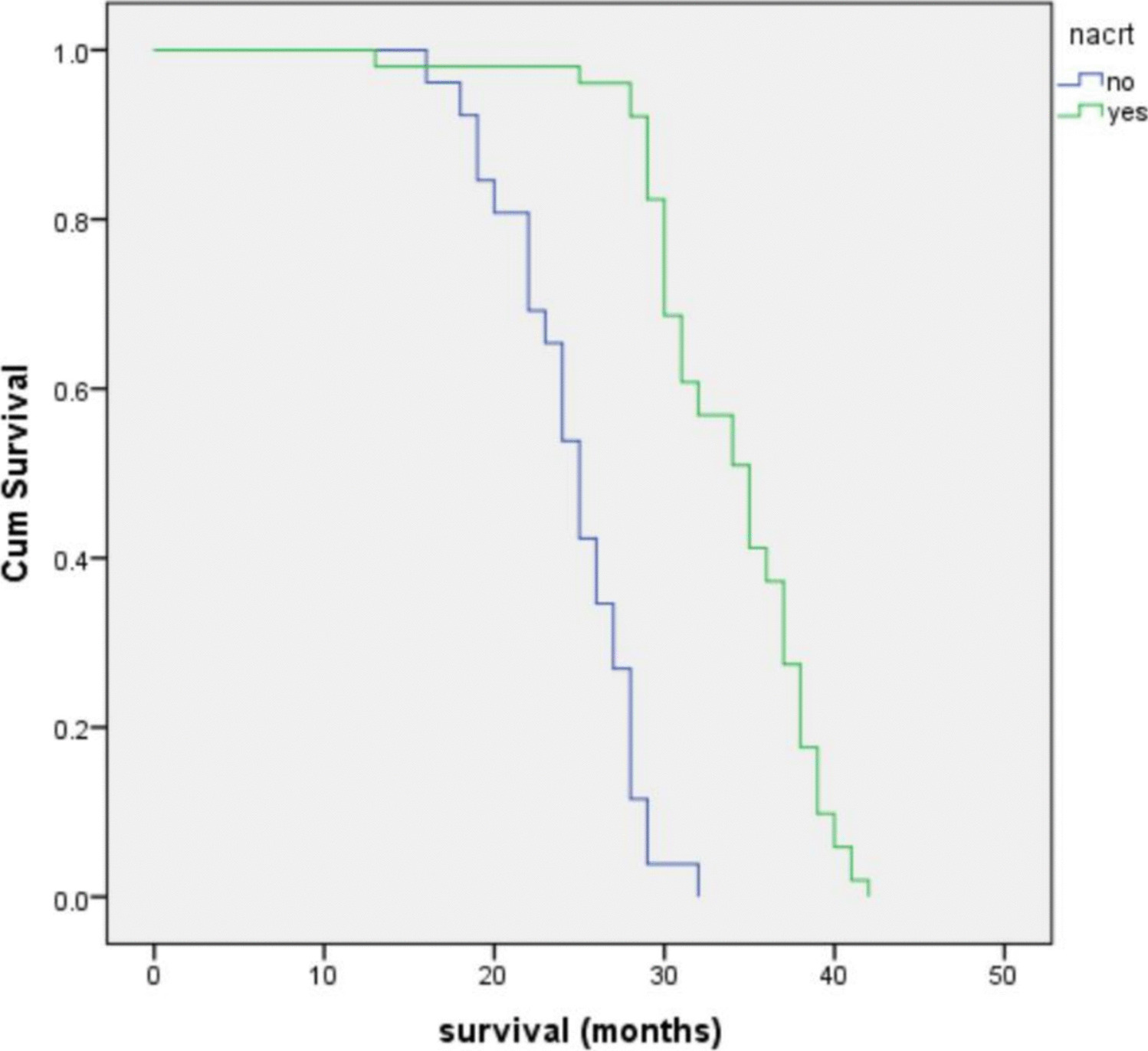
Unfortunately, while endoscopic and organ sparing treatments are the norm globally, most of our patients needed rectal resections and systemic treatment. Locally advanced disease with larger tumours, frequently invading muscularis propria, necessitated surgical resection in a significant proportion. The higher proportion of distant metastatic disease and nodal disease is also reflected in a greater number of patients needing surgical management of nodal and liver disease and frequent need for neo-adjuvant and adjuvant treatments. The benefit of neo-adjuvant treatment we experienced in a subset of our patients is mirrored by a national cancer database review from Cleveland clinic as well [24]. In their cohort, neo-adjuvant chemotherapy improved survival to 30.9 months in patients large (≥ 2 cm), cT4, poorly differentiated primary, or metastatic disease.
The survival outcomes observed in this study, with an estimated 100% 5-year OS in grade I and II disease, align with global data. The better survival in Grade II disease (value of 25 th centile being 93 months for Grade II compared to 87 months in Grade I) could represent impact of adjuvant treatment on survival. However, the poorer outcomes for grade III tumours, with a median survival of 74 months, emphasizes the aggressive nature of higher-grade lesions and the urgent need for more effective treatment strategies.
Our study has several strengths. First, to the best of the authors’ knowledge, this is the first study that investigated rectal NETs in the region. The comprehensive evaluation of a large cohort of patients with rectal NETs, the detailed characterization of tumour features, and treatment outcomes provides valuable data regarding the disease in the region addressing a huge knowledge gap in this understudied region. Our findings also show that in patients where multi-modality treatment achieves downstaging, acceptable outcomes can be achieved for some patients with aggressive disease, supporting this approach in patients with advanced disease, where 5-year OS of 40% was achievable.
Apart from obvious limitations of a retrospective study, coming from a single tertiary referral centre, a potential referral bias cannot be excluded, affecting generalizability of the study. The field of neuroendocrine pathology has evolved significantly beyond mere grading. In our cohort, AJCC staging system of respective years was used and synchronisation could not be done. This lack of synchronisation, lack of detailed subclassification of the pathology as per current guidelines, and the detailed immunohistochemistry panel was also not available for all patients and while not included in this analysis, is an area of future research.
As the first study looking at a potentially important health problem, our study can not only be a benchmark for the region but also highlight treatment challenges in the region or similar demographics and socioeconomic characteristics. The finding of a high proportion of Grade II/III disease in our cohort raises concerns regarding possibly aggressive biology of rectal NET in our region, and coupled with greater insulin resistance seen in this region, we believe it should be investigated if our population has a greater susceptibility to rectal NETs.



Comments (0)