Signet ring histology in the Indian subcontinent accounts for more than 10% of all colorectal cancer patients compared to less than 1% in the Western world [3, 15]. The outcome remains dismal, with high recurrence rates and early demise after the detection of recurrence [2]. The role of PET/CT scans and CEA surveillance in this subgroup is uncertain.
Our study shows that despite a low secretory state at baseline, CEA on follow-up of signet ring cancers remains essential, with 67% of non-secretors having rising CEA at recurrence. On the other hand, a negative CEA in secretory patients is reassuring to both patients and doctors, as less than 3% of patients with normal CEA recur.
In colorectal cancer in general, intensive surveillance protocols following curative resection have demonstrated associations with improved overall survival rates and increased resection rates for recurrent disease, particularly by enhancing the detection of asymptomatic recurrences amenable to surgical intervention [16].
Carcinoembryonic antigen (CEA), discovered by Gold et al. in 1965, is an important prognostic biomarker for monitoring treatment and predicting recurrence in colorectal cancer (CRC) [17]. Elevated preoperative CEA levels are associated with an increased relative risk of recurrence [18].
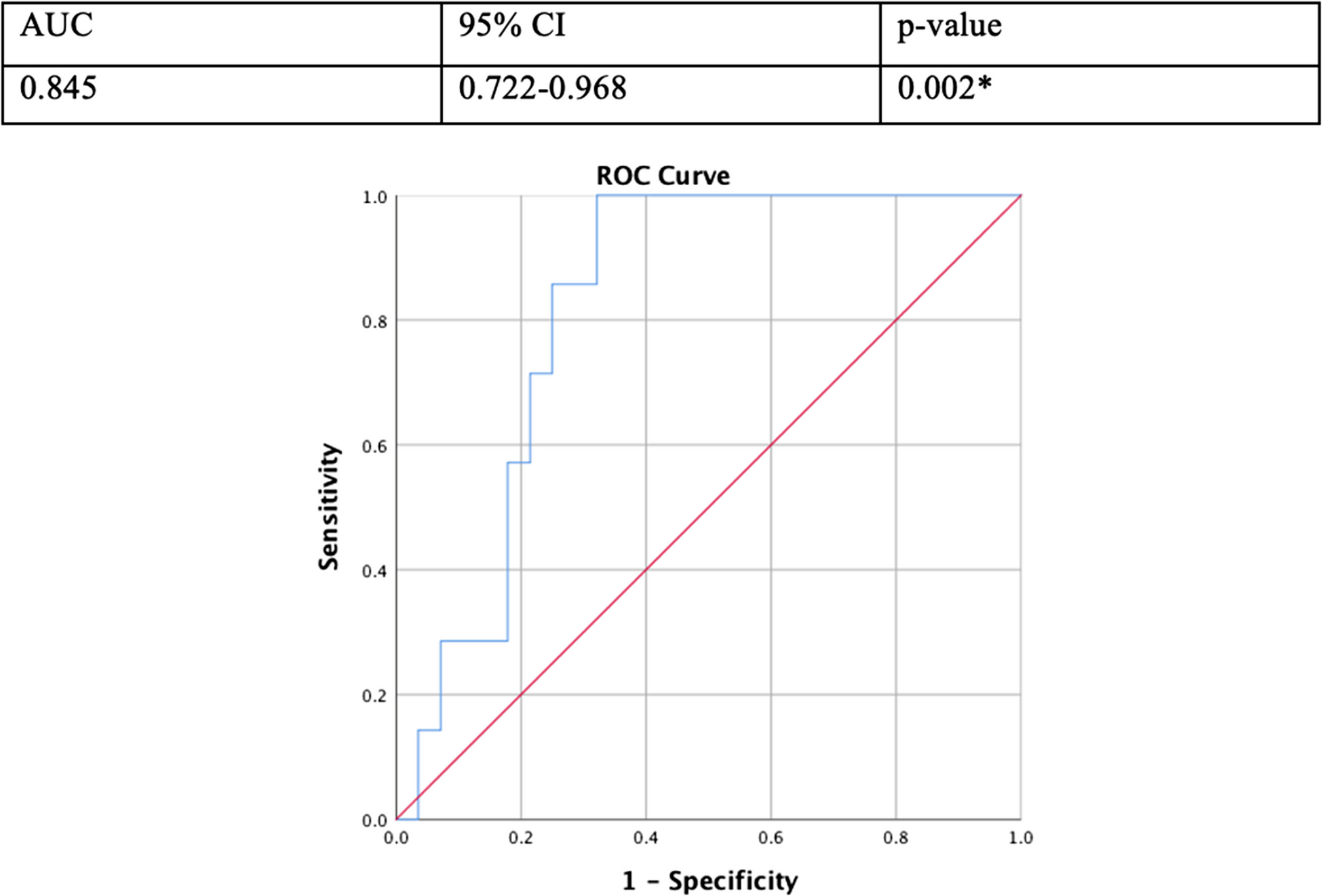
CEA is pivotal in detecting asymptomatic recurrence, accounting for approximately 63% of recurrent CRC cases. In patients with elevated CEA levels but no apparent structural disease on PET/CECT imaging, a CEA threshold of 10 ng/ml and a 1.36-fold increase in CEA value over 3 months significantly predict future recurrence, with respective sensitivities and specificities of 80% and 70% [19].
Preoperative CEA levels influence CEA levels post-curative resection and recurrence rates. Among individuals with baseline CEA levels exceeding 5 ng/ml (secretors), a return to baseline levels post-resection correlates with prolonged time to recurrence. In a retrospective analysis conducted by Holt et al., encompassing 186 patients diagnosed with colorectal cancers (CRCs), 21.5% of the cohort were initial secretors. Among baseline secretors, 66% exhibited elevated levels of CEA at recurrence, while 50% of non-secretors showed a similar elevation. This study revealed a significant association between CEA elevation and CRC recurrence, irrespective of the patient’s initial secretor status [20]. In another study by Chong et al., in 699 cases of colorectal cancer recurrence, baseline secretors constituted 49.5%, and 50.5% were non-secretors. During follow-up, all non-secretors and 58% of secretors achieved a CEA < 5 µg/L. A new rise in CEA to > 5 µg/L prior to relapse was observed in 51% of all patients. This new rise was more likely to be observed among patients whose initial primary was secretory (p < 0.01) [10]. Preoperative CEA levels prior to initial surgery influence CEA dynamics post-curative resection in patients with recurrent colorectal cancer.
Our study was derived from the observation that many signet cell colorectal cancers presented with an elevated CEA at recurrence, irrespective of pretreatment CEA values. With the present cohort, we aimed to understand the pattern of CEA and the sites of relapses in recurrent signet ring cell colorectal cancers.
The role of CEA secretor status and correlation with recurrence has not been studied in signet cell colorectal adenocarcinoma patients. With our investigation, we endeavor to explore the non-secretor to secretor transformation rate in recurrent signet cell colorectal cancers.
Within our study cohort, comprising non-metastatic signet cell colorectal cancer patients, we observed that 32% exhibited baseline carcinoembryonic antigen (CEA) secretory state, defined as CEA levels exceeding 5 ng/ml.
Our findings elucidate a prevalent occurrence of CEA elevations in most recurrent cases, regardless of the baseline secretor status. Specifically, 94.3% of baseline secretors and 67.7% of non-secretors manifested CEA elevation upon recurrence. A small subset of baseline secretors (5.7%) did not display elevated CEA levels at recurrence. Conversely, a substantial proportion of non-secretors presented with elevated CEA at recurrence (much more than the previously reported trials on all colorectal cancers), emphasizing its relevance in surveillance, irrespective of baseline CEA values, even in signet cell colorectal cancers.
Moreover, we investigated the association between CEA secretor status and the site of recurrence (local, peritoneal, systemic), revealing no significant correlation. This result suggested a non-site-specific nature of CEA elevation. This result correlated with a study by Shin et al., where no differences between the different CEA groups were noted regarding the site of recurrence in terms of locoregional and distant metastasis.
Although our study contributes valuable insights, certain limitations warrant acknowledgement. Specifically, our inclusion criteria encompassed all patients with histological evidence of signet cells, regardless of the proportion, deviating from the WHO definition requiring > 50% presentation of signet cells histologically. Additionally, while our sample size surpasses previous studies in recurrent signet cell CRCs, it remains modest. Furthermore, limited documentation of cases in the early years and unavailable CEA trends at recurrence for most cases constitute notable limitations.
In essence, our study underscores the diagnostic importance of CEA levels at recurrence in signet cell colorectal cancer, reinforcing the routine assessment of CEA in follow-up evaluations for this subgroup of patients, regardless of baseline secretor status.



Comments (0)