Predicting Anastomotic Leak in Left-sided Colorectal Cancer Surgery: A Prospective Study Using the Colon Leakage Score
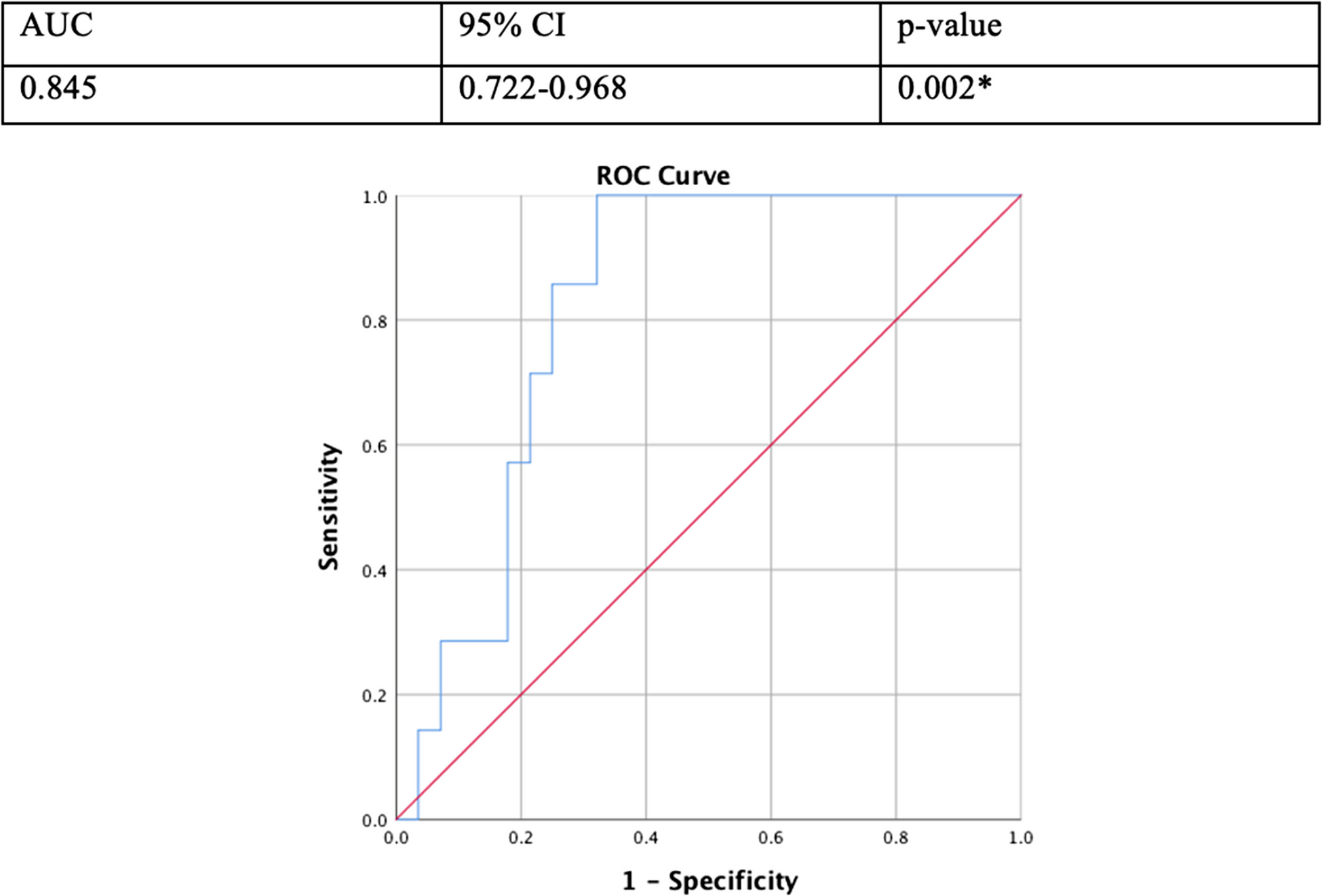
Anastomotic leak (AL) is a serious complication of colorectal surgery, occurring in 3–15% of patients undergoing elective left-sided resections, and is associated with significant morbidity, mortality, and healthcare costs. The Colon Leakage Score (CLS) has emerged as a promising predictive tool for AL, integrating factors such as age, comorbidities, tumor location, and surgical approach. This study aimed to validate the CLS in predicting AL in patients undergoing elective left-sided colorectal surgery. This prospective observational study was conducted at a single tertiary care center from 2020 to 2023 and included 62 patients undergoing elective left-sided colorectal surgery. The CLS was calculated preoperatively using a standardized scoring system. The primary outcome was the incidence of AL, defined as clinical or radiologic leaks. Diagnostic performance of the CLS was evaluated using ROC curve analysis, with sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), accuracy, and area under the curve (AUC) calculated. A cutoff value was determined using Youden’s index. The mean age of participants was 59.8 ± 9.73 years, with 64.5% undergoing laparoscopic surgery. AL occurred in 8.1% of patients, with 83.3% of these having a CLS > 9. The CLS demonstrated high diagnostic performance, with sensitivity of 83.3%, specificity of 91.1%, PPV of 50.0%, NPV of 98.1%, and overall accuracy of 90.3% (p < 0.001). The AUC was 0.912, indicating strong predictive strength. Management of AL included conservative approaches in 6.5% of cases and re-exploration in 3.2%, with an in-hospital mortality rate of 1.6%. The CLS is a robust predictive tool for AL, with a cutoff > 9 showing high sensitivity, specificity, and accuracy. Its ability to stratify risk and guide postoperative management highlights its potential to reduce AL-related morbidity and improve surgical outcomes. However, the study’s single-center design, small sample size, and low AL rate limit generalizability. Further validation in larger, diverse cohorts is needed to confirm its clinical utility and applicability in guiding decisions such as diverting ileostomy. The CLS represents a valuable step toward personalized risk assessment in colorectal surgery.



Comments (0)