
Remember me


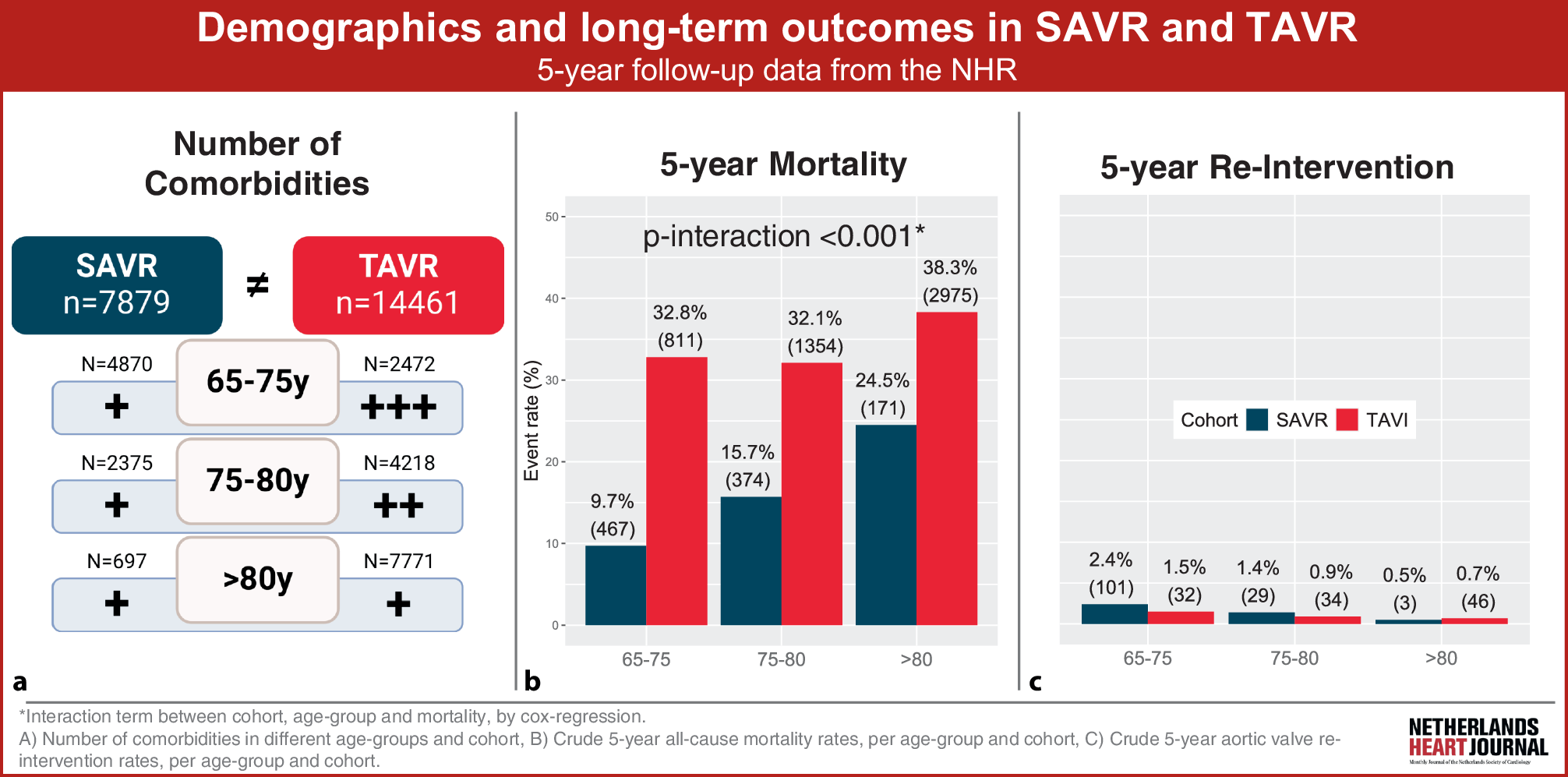
We included 7879 patients who underwent an isolated SAVR procedure and 14,461 patients who underwent an isolated TAVI procedure in the Netherlands in the period 2013–2021. At baseline, SAVR patients were younger than TAVI patients (median age: 73.0 years; IQR: 69.0–77.0 vs 81.0 years; IQR: 77.0–84.0; p < 0.001), were less frequently female (3447 (43.7%) vs 7232 (50.0%); p < 0.001) and had a higher median BMI (27.3 kg/m2; IQR: 24.7–30.4 vs 26.5 kg/m2; IQR: 23.9–29.8; p < 0.001), a lower NYHA class (class III/IV: 1894 (31.7%) vs 7712 (57.6%); p < 0.001) and lower median EuroSCORE II (1.44; IQR: 1.08–2.13 vs 3.25; IQR: 2.01–5.45; p < 0.001) (Tab. 1). After dividing patients into age groups (65–75, 75–80 and > 80 years old), there was no statistically significant difference in the distribution of sex by age, but TAVI patients consistently had a higher NYHA class, a higher rate of poor mobility and a higher EuroSCORE II compared with SAVR patients (see Table S1 in Electronic Supplementary Material).
Table 1 Baseline characteristicsTAVI patients showed higher prevalences of COPD, diabetes, AF, dialysis, previous stroke, unstable angina and recent MI than SAVR patients. In addition, they had more frequently undergone previous cardiac surgery, had higher creatinine levels, lower LVEF and higher PASP. After stratifying patients by age, these higher rates in TAVI remained statistically significant, except for diabetes and dialysis in the older age group. SAVR patients, on the other hand, had higher rates of endocarditis, a critical pre-operative condition and higher urgency, which were consistent through all age groups. Tables S2 and S3 in the Electronic Supplementary Material show baseline characteristics of both TAVI and SAVR cohorts in early (2013–2016) and recent (2017–2021) years. Several changes in baseline characteristics were observed over time, which were largely similar between TAVI and SAVR cohorts. Regarding trends in older age groups, the proportions of female sex, age and EuroSCORE II increased in older age groups in both cohorts. The prevalences of COPD, AF, dialysis, recent MI and previous cardiac surgery declined in older age groups in both cohorts and thus were highest in younger age groups (see Table S4 in Electronic Supplementary Material).
In SAVR patients, the prevalence of NYHA class III/IV increased with higher age (p for trend < 0.001), while it did not change and remained high in all age groups for TAVI patients. Rates of poor mobility, diabetes, previous stroke, recent MI, critical pre-operative condition and urgency decreased in older age groups for TAVI patients, while this was not the case for SAVR patients. LVEF increased across age groups in TAVI patients but not in SAVR patients PASP increased in subsequent age groups for both cohorts.
Mortality and aortic valve re-intervention at 5-year follow-upAfter a median follow-up time of 1617 days, 1012/7879 (12.8%) SAVR patients died. In contrast, after 1121 days of follow up, 5140/14,461 (35.5%) TAVI patients died (Tab. 2). Median survival was shorter after TAVI (685 days; IQR: 250–1160 vs 874 days; IQR: 317–1356; p < 0.001 (Fig. 2)). This trend was also seen in both early and recent years (see Tables S2 and S3 in Electronic Supplementary Material) and when including only transfemoral TAVI patients versus SAVR patients (see Table S5 in Electronic Supplementary Material). However, there was no interaction between time, cohort and outcomes (see Table S6 in Electronic Supplementary Material). Aortic valve re-intervention rates were low (135 (1.9%) in SAVR patients vs 114 (0.9%) in TAVI patients; p < 0.001), and the time to aortic valve re-intervention was shorter in TAVI compared with SAVR (52 vs 338 days; p < 0.001).
Fig. 2
Kaplan–Meier survival curves of 5‑year mortality after surgical aortic valve replacement (SAVR) versus transcatheter aortic valve implantation (TAVI). a Total cohort, b SAVR-treated patients only, stratified by age group, c TAVI-treated patients only, stratified by age group, d youngest age group (65–75 years), stratified by cohort, e middle age group (75–80 years), stratified by cohort, and f oldest age group (> 80 years), stratified by cohort
Comparing TAVI and SAVR patients who died during follow-up, showed that TAVI patients were older and more frequently female and had lower BMI, more often NYHA class III/IV at the time of the procedure, poor mobility and higher EuroSCORE II (see Table S7 in Electronic Supplementary Material). TAVI patients who had died had a higher prevalence of chronic lung disease, AF, stroke and previous cardiac surgery. LVEF was lower in TAVI patients, whereas PASP was higher. SAVR patients, in contrast, more frequently were in critical pre-operative condition and had previous thoracic aortic surgery and higher urgency.
Outcomes stratified by ageMortality rates increased with increasing age for both procedures, but this was more pronounced after SAVR than TAVI (9.7% for 65–75 years, 15.7% for 75–80 years and 24.5% for > 80 years in SAVR; p < 0.001, compared with 32.8%, 32.1% and 38.3%, respectively, in TAVI; p < 0.001) (Tab. 3, and see Tables S8 and S9 in Electronic Supplementary Material). Interaction analysis between cohort and age group revealed that the hazard associated with TAVI decreased relative to SAVR in higher age groups (see Table S10 in Electronic Supplementary Material). Aortic valve re-intervention rates were low and declined with increasing age (2.4%, 1.4% and 0.5% in SAVR; p < 0.001, compared with 1.5%, 0.9% and 0.7% in TAVI; p < 0.001).
Table 3 Outcomes per age group
Comments (0)