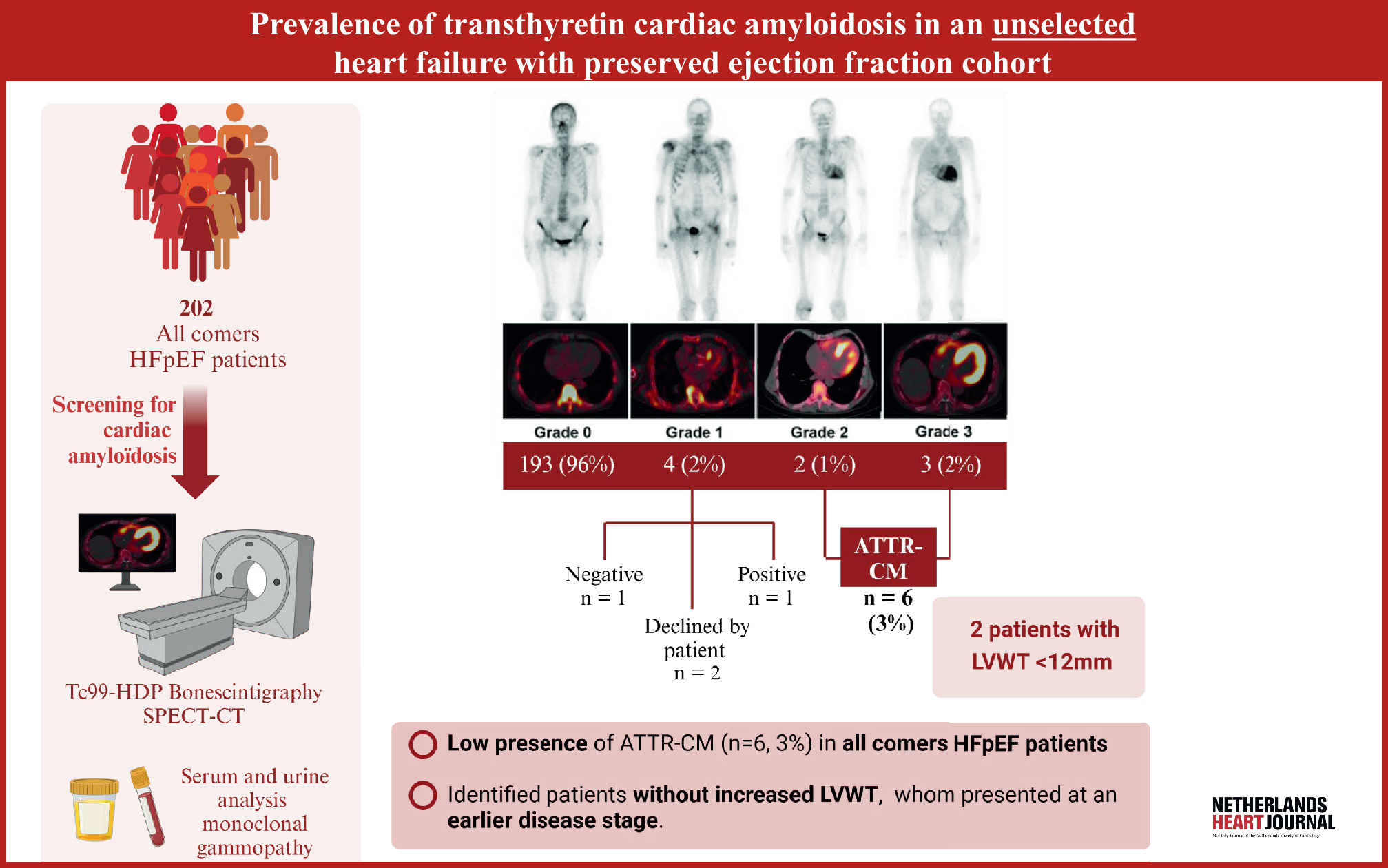
Current guidelines recommend active screening for ATTR-CM in HFpEF patients with unexplained LVWT ≥ 12 mm and ≥ 1 typical red flags for amyloid cardiomyopathy [7]. In light of this directive, our study has several noteworthy findings.
First, we found an ATTR-CM prevalence of 3% in an unselected HFpEF cohort, which is lower than that previously reported [1,2,3, 20]. This can be attributed to the fact that previous studies primarily included HFpEF patients with LVWT ≥ 12 mm [1,2,3], thereby selecting a subgroup with a higher ATTR-CM prevalence. The study by Healy et al. is one of only 2 studies that included HFpEF patients without explicitly increased wall thickness [20]. However, even in their cohort, 62% of the patients had LVWT ≥ 12 mm (median: 12 mm). The other study, by Devesa et al., included hospitalised HFpEF patients with LVWT < 12 mm and reported an ATTR-CM prevalence of 5% [5]. In our outpatient clinic, we included both HFpEF patients with and without LV hypertrophy but found an even lower ATTR-CM prevalence. This may be partly explained by the fact that 64% of our patients were female, whereas ATTR-CM is known to be more common in men [21]. Initially, there was concern that female patients with ATTR-CM are underdiagnosed [21], but our findings do not support this hypothesis. Despite screening a large proportion of women, we identified very few cases of ATTR-CM. The high representation of female patients in our HFpEF cohort may therefore contribute to the low ATTR-CM prevalence observed.
Second, we identified 2 ATTR-CM patients (33%) without increased LVWT, who were in an early disease stage, as shown by their NAC prognostic stage and NYHA class. This supports the concept that cardiac uptake on bone scintigraphy serves as an indicator of ATTR-CM presence rather than amyloid fibril quantity and may thus identify ATTR-CM before clinically evident LV hypertrophy [5, 10]. If we had followed the current guidelines, these patients would have been overlooked or diagnosed at a later disease stage [7]. Consequently, to facilitate early ATTR-CM diagnosis, it may be necessary to broaden the scope beyond patients with increased LVWT and consider other patient groups as well.
Currently, there is a strong focus on using HFpEF patients as a screening group for ATTR-CM [7]. However, it is well established that over half of the ATTR-CM patients have a reduced or mildly reduced LVEF [22]. This underscores that ATTR-CM can manifest across various cardiology subgroups, highlighting the urgent need for diagnostic indicators beyond echocardiography.
Last, we observed a high prevalence of typical red flags for ATTR-CM in all HFpEF patients. Specifically, 81% of all HFpEF patients exhibited ≥ 1 red flags indicative of ATTR-CM. These findings highlight the diagnostic challenge for ATTR-CM, particularly in early disease stages. Routine bone scintigraphy in an unselected HFpEF population remains controversial due to the low prevalence of ATTR-CM in this group and the significant number of scans required. Therefore, we do not recommend standardised screening for ATTR-CM in all HFpEF patients but emphasise the urgent need for more specific ATTR-CM indicators beyond the currently described red flags and echocardiographic parameters. Meanwhile, targeted screening of HFpEF patients using existing screening tools may be a practical approach in clinical practice [13], as screening remains essential, particularly with the increasing number of treatment options available, even for patients in advanced disease stages [23].
Study limitations
Our results may be affected by selection bias as the entire patient cohort was predominantly referred by cardiologists, with only a small proportion referred by general practitioners. However, our hospital functions as both a regional and university hospital, catering to a diverse patient population representative of the local community. We believe our cohort broadly reflects the HFpEF population, as all patients suspected of HFpEF are evaluated systematically, irrespective of LVWT or ATTR-CM–related red flags. Nonetheless, we acknowledge that the specialised nature of our HFpEF clinic and the diagnostic expertise of referring cardiologists may introduce a degree of pre-selection bias, potentially impacting the ATTR-CM prevalence. Moreover, the high proportion of female patients in our cohort may have contributed to the low prevalence of ATTR-CM observed.
Furthermore, the decision of 2 patients to decline further evaluation for ATTR-CM following inconclusive bone scintigraphy may have influenced the ATTR-CM prevalence in our cohort, particularly given its already low rate. Nonetheless, we believe that the clinical relevance of these 2 cases is limited considering the overall very low prevalence of ATTR-CM in an unselected HFpEF cohort. Therefore, we excluded these patients from further analyses.



Comments (0)