
Remember me









IBA is a salt formulation combining racemic ibuprofen with l-arginine, an amino acid that enhances gastrointestinal solubility without altering the drug’s mechanism of action. The addition of arginine enhances the solubility and absorption of ibuprofen [16, 53]. An in vitro assessment investigating the intestinal absorption of ibuprofen and IBA, showed that IBA is characterized by a significantly (p < 0.05) faster absorption after 10 min compared to that of the conventional ibuprofen (17.01 ± 0.0.25 × 10–6 cm/s vs. 8.56 ± 0.18 × 10−6 cm/s, respectively). Additionally, IBA showed also a significantly (p < 0.05) higher absorption compared to ibuprofen at 10 min (4.46 ± 0.06 µg vs. 10.59 ± 0.12 µg/min for IBA and 2.11 ± 0.04 µg and 8.97 ± 0.09 µg/min for ibuprofen) (data on file). Clinical studies in healthy volunteers have demonstrated that IBA is absorbed significantly faster than conventional ibuprofen formulations. This enhanced absorption is reflected in a higher peak plasma concentration (Cmax) and a significantly shorter time to maximum concentration (Tmax) across all tested doses, including 200, 400, and 600 mg [53].
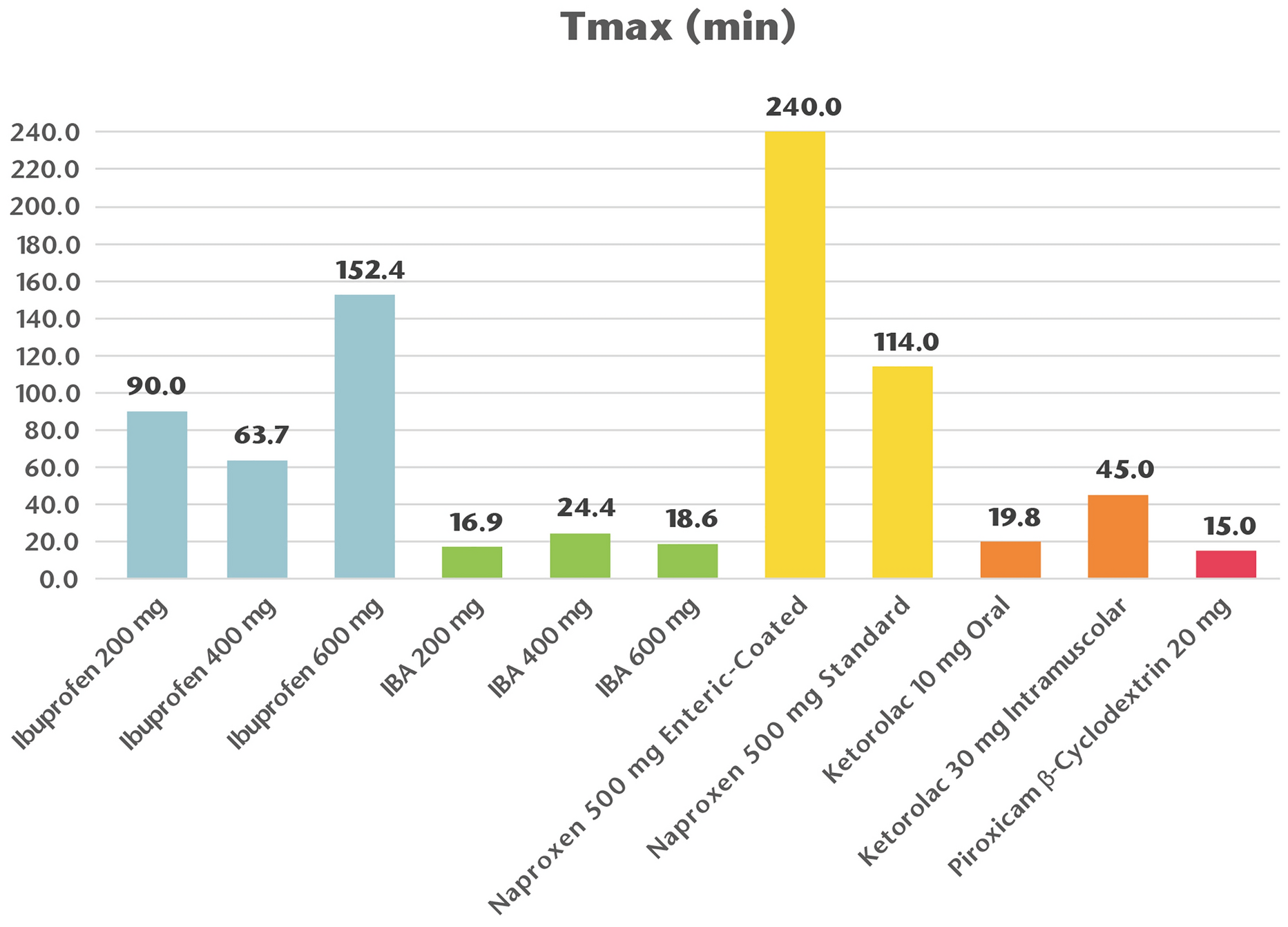
This enhanced pharmacokinetic profile, characterized by higher Cmax and a shorter time to peak concentrations Tmax, ensures a faster onset of pain relief, which is particularly valuable in clinical settings where immediate intervention is required [15, 16]. Notably, when compared to ibuprofen-free acid, IBA reaches peak plasma levels up to 5.5 times faster, indicating a rapid onset of action. Furthermore, plasma concentrations observed as early as 5 min post-administration with IBA are comparable to those reached at 60 min with conventional ibuprofen [53]. A comparative evaluation of time to reach peak plasma concentration is reported in Fig. 1.
Fig. 1
Comparative evaluation of peak plasma concentration. Time to peak drug concentration—Tmax—(in minutes) of various formulations of ibuprofen, ibuprofen arginine (IBA), naproxen, ketorolac, and piroxicam β-cyclodextrin. IBA demonstrates a significantly faster Tmax compared to conventional ibuprofen formulations and other non-steroidal anti-inflammatory drugs (NSAIDs), indicating a more rapid onset of action. The granular soluble form of IBA (200 and 400 mg) exhibits the shortest Tmax values, further supporting its enhanced absorption properties. Data adapted from published pharmacokinetic studies [53,54,55,56]
Once absorbed, IBA undergoes the same metabolic pathways as conventional ibuprofen, ensuring no significant alteration in drug clearance or overall systemic exposure. Despite its faster absorption, the half-life (T1/2) and overall drug exposure (AUC values) remain comparable between the two formulations. Ibuprofen is predominantly metabolized in the liver via cytochrome P450 enzymes (CYP2C8 and CYP2C9), leading to the formation of hydroxylated metabolites that are primarily excreted in urine. Additionally, the chiral nature of ibuprofen plays a crucial role in its metabolism, as the S(+)-ibuprofen enantiomer is responsible for the drug’s anti-inflammatory effects. Importantly, studies confirm that IBA does not alter the stereoselective pharmacokinetics of ibuprofen, ensuring that the active enantiomer remains available in sufficient concentrations to exert its therapeutic effects [53].
Although gastrointestinal complains have been reported as most frequent adverse events [15], the presence of arginine potentially results in a better gastrointestinal tolerance than standard ibuprofen formulation [57]. IBA has been shown to be less gastrolesive than ibuprofen in animal studies [58].
The rapid relief that characterizes IBA is crucial for improving patient comfort, minimizing disruptions to daily activities, and enhancing overall quality of life [15].
By effectively managing acute pain and reducing inflammation at early stage, it is possible to prevent maladaptive changes in pain processing pathways, such as central sensitization, which can lead to persistent pain [59, 60]. IBA’s ability to target the inflammatory component of pain and rapidly reduce pro-inflammatory mediators offers the dual benefits of immediate relief and long-term prevention of chronic pain [59, 61].
Another advantage of IBA is its favorable safety profile, allowing for effective pain relief at lower doses, thereby minimizing the risk of adverse events [15,16,17]. l-Arginine significantly reduces ibuprofen-induced gastric damage in a dose-dependent manner. The gastroprotective mechanism of l-arginine against ibuprofen-induced gastric injury is primarily mediated through the nitric oxide (NO) pathway, which plays a crucial role in maintaining gastric mucosal integrity. l-Arginine serves as a precursor for nitric oxide synthase (NOS), which converts it into NO, a key mediator of gastric mucosal defense. NO enhances mucosal blood flow, ensuring adequate oxygen and nutrient delivery to the gastric lining, which is essential for maintaining epithelial integrity and promoting ulcer healing. Also, NO promotes mucus and bicarbonate secretion, which helps neutralize gastric acid and provides a protective barrier against NSAID-induced injury [17]. Additionally, IBA showed significant potential for the mitigation of cardiovascular toxicity linked to COX-2 inhibitors [62].
In Table 1, we provide a comprehensive summary of the rapid-onset action data derived from key randomized controlled clinical trials (RCTs) that investigated the use of IBA in adult patient populations. These studies specifically evaluated the efficacy and the rapidity of action of IBA, compared with ibuprofen, other NSAIDs, and/or placebo. The RCTs collected data from approximately 1700 patients, providing substantial evidence of IBA’s effectiveness and quick onset of action across various acute and chronic pain conditions, including dental pain, postoperative pain, osteoarticular pain, dysmenorrhea, and tension headaches.
Table 1 Summary of clinical studies evaluating the efficacy and onset of action of ibuprofen arginine (IBA)The Use of IBA in Dental PainIn dental pain, IBA effectively reduces inflammation and swelling following procedures, with a significantly faster onset of pain relief compared with conventional ibuprofen (29–32 min for IBA compared with 44–64 min for ibuprofen) [10, 63,64,65,66]. A randomized, double-blind, placebo-controlled trial assessed the analgesic efficacy, onset of action, and tolerability of IBA (200 and 400 mg) compared to standard ibuprofen (200 and 400 mg) and placebo in 498 patients with moderate-to-severe postoperative dental pain [63]. Meaningful pain relief was achieved significantly faster with IBA (median time: 28–29 min) compared to standard ibuprofen (44–52 min) and placebo (not reached). Within the first hour, 77.6% and 83.7% of patients receiving IBA 200 mg and 400 mg, respectively, reported meaningful pain relief compared to 61.0% and 63.0% for standard ibuprofen and 39.8% for placebo (all, p < 0.05). Pain intensity differences (PID) and total pain relief (TOTPAR) scores were consistently higher for IBA at early time points [54].
Ettlin et al. [64] conducted a randomized, triple-blind, placebo-controlled trial to assess the efficacy of IBA (800 mg) in managing pain during and after scaling and root planning (SRP) in patients with mild-to-moderate chronic periodontitis. Sixty-four patients were randomized to receive either IBA or placebo 30 min before treatment. Pain was measured using numeric and visual analog scales. The results showed that IBA significantly reduced pain during treatment, with a 72% reduction in median pain levels compared to placebo (p = 0.023). The median maximum pain scores were 10 (interquartile range: 4–31) for IBA and 28 (10–50) for placebo. IBA resulted more effective in reducing pain intensity and providing pain relief over the first 6 hours postoperatively. However, post-treatment pain levels were low in both groups, with no significant differences. Additionally, no adverse events were reported [64].
Mehlisch et al. [65] conducted a double-blind, randomized, placebo-controlled trial to compare the analgesic efficacy and onset of action of IBA (200 and 400 mg) to conventional ibuprofen (200 and 400 mg) and placebo in 500 patients with moderate-to-severe postoperative dental pain. Time to meaningful pain relief was significantly shorter with IBA, with median times of 31–32 min compared to 58–64 min for conventional ibuprofen (p < 0.05). Patients receiving IBA reported significantly higher pain relief scores (TOTPAR: 13.3–13.6 vs. 10.0–12.4 for conventional ibuprofen) and faster onset of action. IBA also prolonged the duration of analgesia, with a longer median time to re-medication (4.4–4.5 h vs. 3.8–4.2 h for conventional ibuprofen). Both formulations were well tolerated, with similar adverse event rates across all groups [65].
Lastly, Desjardins et al. [66] conducted a randomized, double-blind, placebo-controlled trial to evaluate the efficacy and onset of action of IBA (200 and 400 mg) compared with standard ibuprofen (200 and 400 mg) and placebo in 226 patients with postoperative dental pain following third molar extraction. Patients receiving IBA 400 mg achieved meaningful pain relief significantly faster (median time: 24 min) compared to ibuprofen 400 mg (48 min) and placebo (not reached, p < 0.05). TOTPAR scores for IBA were significantly higher than those for standard ibuprofen, particularly at early time points. Peak plasma ibuprofen concentrations were reached more rapidly with IBA than with standard ibuprofen, confirming its faster absorption. Both formulations were well tolerated, with no significant differences in adverse events [66].
Recently, a randomized, triple-blind, placebo-controlled clinical trial aimed to evaluate the effectiveness of a novel desensitizing gel containing IBA in mitigating bleaching-induced tooth sensitivity. Sixty-two participants with upper canines of shade A2 or darker were randomly assigned to receive either the experimental ibuprofen/arginine gel or a placebo. The gel was applied topically for 15 min prior to bleaching with 35% hydrogen peroxide. Tooth sensitivity was assessed using visual analog scales (VAS) and numerical rating scales (NRS) at multiple time points up to 48 hours post-bleaching. Color change was evaluated using Vita Classical, Vita Bleachedguide, and Vita EasyShade shade guides. The results demonstrated that the application of ibuprofen/arginine gel significantly reduced the risk (odds ratio = 0.14; p = 0.004) and intensity (p < 0.005) of bleaching-induced tooth sensitivity without compromising bleaching efficacy (p > 0.05) [67].
IBA in Postoperative PainPostoperative pain management remains a crucial aspect of recovery after surgery [68]. A randomized, double-blind, placebo-controlled trial aimed to evaluate the analgesic efficacy and tolerability of oral IBA (400 mg) compared to intramuscular (IM) magnesic dipyrone (2 g) and placebo in 106 patients (62 years mean age) experiencing moderate-to-severe postoperative pain after total hip replacement surgery. Pain intensity was assessed using a 100-mm visual analog scale (VAS) at multiple time points (baseline, 10–300 min post-administration). Both active treatments demonstrated significant pain relief, reducing baseline pain levels by approximately 70% at the study’s conclusion. The onset of analgesia was rapid, with a 50% reduction in pain intensity within the first hour. While both active treatments were significantly more effective than placebo, no statistically significant differences were observed between IBA and dipyrone. The need for rescue medication was comparable across groups, and patient satisfaction was notably higher in the active treatment groups compared to placebo (56% for IBA, 66% for dipyrone, and 21% for placebo). Tolerability was excellent, with only two reported adverse events (headache), one in the IBA group and one in the placebo group [68].
A randomized, double-blind, double-dummy, single-dose, parallel-group study conducted at two medical centers. A total of 120 patients undergoing elective orthopedic procedures were recruited and randomized into three treatment groups: IBA (400 mg) orally plus placebo IM., morphine sulfate (5 mg) IM plus placebo orally and morphine sulfate (10 mg) IM plus placebo orally. Pain intensity and relief were assessed using VAS and Verbal Rating Scores (VRS) at multiple time points up to 240 min post-administration. Patients included in the study were 18–75 years old (mean age: 40–45 years), classified I or II according to The American Society of Anesthesiologists (ASA) Physical Status Classification, and had undergone orthopedic procedures of varying complexity (minor, intermediate, or major surgeries). All participants had moderate to severe postoperative pain at the time of randomization. The study demonstrated that all three treatment groups—IBA (400 mg), morphine 5 mg, and morphine 10 mg—produced significant pain reduction compared to baseline. Despite differences in administration routes (oral vs. intramuscular), no statistically significant differences were observed in overall pain relief or peak analgesic effect among the groups. Additionally, the time to request additional analgesia was similar across treatments, indicating that IBA provided a duration of pain relief comparable to morphine. One of the key objectives of this study was to assess whether IBA could serve as an effective morphine-sparing alternative. The results showed that approximately 50% of patients in both the IBA and morphine 5 mg groups required additional analgesia, compared to 40% in the morphine 10 mg group. However, this difference was not statistically significant (p > 0.05). The similar rate of rescue medication use across all groups reinforces IBA provided pain control on par with intramuscular morphine. IBA was found to have a favorable safety profile, with no significant differences in the incidence of adverse events across treatment groups. The most commonly reported adverse events were nausea and vomiting, occurring in a small proportion of patients. Patient-reported satisfaction with pain relief was similar across treatment groups, with 44% of patients in the IBA group, 41% in the morphine 5 mg group, and 58% in the morphine 10 mg group rating their pain relief as “good” or better. Although the highest satisfaction was reported in the morphine 10 mg group, the differences were not statistically significant (p > 0.05) [69].
Postoperative pain following cesarean section is a significant concern, as it impacts maternal mobility, recovery, and the ability to care for the neonate. Effective pain relief strategies must balance efficacy, safety, and convenience, particularly for breastfeeding mothers where opioid use is often limited. A single-center double-blind, double-dummy, placebo-controlled study enrolling 92 women undergoing elective cesarean section and randomized into three treatment groups: IBA 400 mg orally plus placebo IM, ketorolac 30 mg IM plus placebo orally and placebo orally plus placebo IM. Pain intensity was assessed using a 100-mm VAS at multiple time points (15, 30, 45, 60, 90, 120, 180, 240, 300, and 360 min post-dosing). Rescue medication (IM ketoprofen 100 mg) was permitted if pain relief was inadequate. At the beginning of the study, pain intensity was comparable across all groups, with baseline scores on the VAS ranging from 78 to 81 mm. Following administration of the study medications, both IBA and ketorolac produced significant pain reduction compared to placebo (p < 0.001). By 60 min post-dosing, pain levels had decreased substantially in both active treatment groups, reaching 47 mm in the IBA group and 48 mm in the ketorolac group. In contrast, the placebo group exhibited a temporary pain reduction to 63 mm, but pain intensity increased again, stabilizing around 69 mm. The pain relief trajectories of IBA and ketorolac were nearly identical. The need for additional analgesia was higher in the placebo group, with 66% of patients requiring rescue medication compared to 43% in the IBA group and 37% in the ketorolac group. The time before requesting rescue medication was also significantly longer in both active treatment groups compared to placebo (p < 0.05), reinforcing their superior analgesic efficacy. However, there was no statistically significant difference between IBA and ketorolac in terms of rescue medication requirements, further supporting their comparable effectiveness. Patient-reported satisfaction was notably higher in the active treatment groups compared to placebo. Nearly half of the patients (47%) in the IBA group and 53% in the ketorolac group rated their pain relief as “good” or better, while only 12% of placebo-treated patients reported a satisfactory response (p < 0.05). Despite ketorolac showing a slightly higher satisfaction rate, the difference between IBA and ketorolac was not statistically significant, indicating comparable patient-perceived efficacy. Finally, safety profile of both active treatments was favorable, with no adverse effects reported during the six-hour study period. Importantly, IBA demonstrated a tolerability profile comparable to ketorolac, reinforcing its suitability as a safe and effective non-opioid analgesic for post-cesarean section pain management [70].
Postoperative pain following suction termination of pregnancy is a significant concern, influenced by physiological and psychological factors. A randomized, double-blind, placebo-controlled study was conducted in a parallel-group design to evaluate the efficacy and safety of preoperative IBA (400 mg) compared to placebo for postoperative pain control in patients undergoing suction termination of pregnancy. A total of 75 women aged 16–45 years undergoing first-trimester suction termination of pregnancy were enrolled. Patients were randomly assigned to receive a single oral dose of IBA (400 mg) or placebo 30 min before surgery. Pain intensity was assessed using a 100-mm VAS at baseline (preoperatively) and at multiple time points (30, 45, 60, 90, 120, 180, and 240 min postoperatively). The primary endpoint was the area under the curve (AUC) of the VAS scores over time, which reflects overall pain burden. Patients who received IBA experienced significantly lower postoperative pain levels compared to those in the placebo group (p < 0.02). This difference was particularly evident when analyzing the area under the pain score vs. AUC, which was 649 mm-min for IBA, compared to 1961 mm-min for placebo (p < 0.02). Furthermore, the mean peak pain intensity recorded throughout the study was significantly lower in the IBA group, with a peak VAS score of 10 mm, compared to 26 mm in the placebo group (p < 0.002). Similarly, when considering the total sum of VAS scores across all time points, the IBA group demonstrated consistently lower pain levels (23 mm vs. 78 mm for placebo, p < 0.002). Also, IBA provided sustained pain relief, as evidenced by consistently lower pain scores at 30, 45, 60, 90, and 120 min postoperatively compared to placebo. Beyond 180 min post-surgery, pain intensity declined in both groups, indicating a natural physiological reduction in postoperative pain as part of the recovery process. However, the overall pain burden remained significantly lower in the IBA group. Importantly, no patient in either treatment group required additional analgesia during the four-hour study period. IBA was well tolerated, with no clinically significant adverse events reported [71].
IBA in Osteoarticular PainIn osteoarticular pain caused by osteoarthritis or rheumatoid arthritis, IBA relieves pain and improves joint function. The granular soluble form (in sachets) provides significantly faster and more potent analgesic effects compared to tablets, as shown in a single-dose, double-blind, crossover study [72]. The study investigated the pharmacokinetics and analgesic efficacy of the granular soluble form of IBA (200 mg and 400 mg sachets) in comparison with traditional tablets. In healthy volunteers, the granular form showed significantly faster absorption and higher plasma bioavailability within the first hour after administration. Peak plasma concentrations were higher for the sachets (200 mg: 26.1 µg/ml; 400 mg: 56.4 µg/ml) compared to tablets (200 mg: 16.3 µg/ml; 400 mg: 43.0 µg/ml). Time to peak concentration was substantially shorter for the sachets (200 mg: 16.9 min; 400 mg: 24.4 min) versus tablets (200 mg: 90.0 min; 400 mg: 63.7 min). This rapid onset of action is attributed to the enhanced absorption rate of granular formulation [58].
IBA in Muscle Tension Headaches and MigraineSimilarly, IBA alleviates muscle tension for tension headaches and reduces pain intensity, improving the likelihood of being pain-free at 2 h for patients with frequent episodic tension-type headaches and moderate or severe pain [73]. Tension-type headaches, characterized by bilateral, pressing, or tightening pain, are among the most common primary headache disorders, often leading to significant discomfort and functional impairment [74].
A double-blind, cross-over trial was conducted to compare the efficacy and tolerability of IBA (400 mg), β-cyclodextrin piroxicam (20 mg), and placebo for the treatment of tension-type headache. Thirty patients with recurrent tension-type headaches were randomized to receive a single dose of each treatment during three separate headache episodes. Pain intensity was assessed using a 100-mm VAS at baseline and multiple intervals post-dosing (15–240 min). IBA and β-cyclodextrin piroxicam significantly reduced pain intensity compared to placebo, with mean AUC for VAS scores of 28 mm for IBA, 41 mm for β-cyclodextrin piroxicam, and 4 mm for placebo (p < 0.01 for IBA vs. placebo). A significantly greater number of patients rated pain relief as complete or considerable with IBA and β-cyclodextrin piroxicam (38.5% respectively) compared to placebo (15.4%; p < 0.02). Both treatments were well tolerated, with only two reports of nausea which were not considered treatment-related [10, 73].
A randomized, parallel-group, double-blind, double-dummy, placebo-controlled study has been conducted to assess the onset of action and efficacy of IBA compared to ibuprofen and placebo in patients experiencing acute tension headache. The primary objective was to determine which treatment offered faster and more effective pain relief. The study demonstrated that both IBA and ibuprofen were effective in reducing headache intensity when compared to placebo. However, IBA exhibited a faster onset of pain relief, suggesting a potential advantage over standard ibuprofen formulations. Within 30–45 min post-treatment, a higher proportion of patients in the IBA group reported meaningful pain relief. Also, the peak analgesic effect was comparable between IBA and ibuprofen, as well as their favorable tolerability profile [74].
Moreover, Sandrini et al. conducted a multicenter, double-blind, randomized, placebo-controlled study aimed to evaluate the efficacy and safety of IBA (400 mg) in migraine treatment, particularly its ability to provide early pain relief. The study enrolled 40 patients with diagnosed migraine. Each participant was treated with a single oral dose of IBA (400 mg) or placebo during two consecutive migraine attacks in a cross-over design, ensuring that each patient served as their own control. The primary endpoints included a pain relief at 30 min post-treatment, the reduction in pain intensity at 1, 2, 4, and 6 h post-administration and tolerability and safety assessment. The study demonstrated that IBA provided significant pain relief as early as 30 min after administration (p < 0.05). This early onset of action confirms the advantage of IBA over conventional ibuprofen formulations, which typically have a slower absorption rate. Moreover, the pain intensity reduction remained statistically significant at 1, 2, 4, and 6 h post-treatment (p < 0.001) when compared to placebo. These findings indicate that IBA not only acts quickly but also provides sustained relief throughout the acute migraine episode. Finally, IBA was well tolerated, with no reports of serious adverse events during the study period [75].
IBA in DysmenorrheaPrimary dysmenorrhea, characterized by lower abdominal cramp-like pain associated with menstruation, significantly impacts quality of life. NSAIDs are the first-line treatment, but their onset of action varies [76]. A randomized, cross-over, double-blind, placebo-controlled trial has been conducted to compare the onset and efficacy of IBA against ibuprofen and placebo, assessing their ability to provide rapid and effective pain relief. The study enrolled 99 patients with a confirmed history of moderate-to-severe primary dysmenorrhea. Each participant underwent three treatment periods, receiving a single or double dose of IBA, ibuprofen or placebo in a random sequence. A washout period was implemented between treatments to prevent carryover effects. Pain intensity and pain relief were measured at frequent intervals post-administration using validated pain assessment tools, including a VAS scale ranging from 0 (no pain) to 100 mm (worst imaginable pain), a categorical Pain Relief Scores and a Time to First Perceptible and Meaningful Pain Relief (TmaxPR and TmaxMPR). The study demonstrated that both IBA and ibuprofen were significantly more effective in reducing menstrual pain compared to placebo. However, a key distinction emerged in the onset of action: IBA provided faster pain relief, with patients experiencing the first signs of improvement earlier than those receiving ibuprofen. Within 30–45 min post-dosing, a greater proportion of individuals in the IBA group reported meaningful pain relief, indicating a quicker response compared to ibuprofen. In terms of overall efficacy, both IBA and ibuprofen achieved similar levels of peak pain relief, suggesting that while the speed of action differed, their maximum analgesic effects were comparable. In contrast, the placebo group showed minimal pain reduction, reinforcing the robustness of the study design and the clear efficacy of the active treatments. Regarding safety and tolerability, both IBA and ibuprofen were well tolerated, with no reports of serious adverse events. The most commonly observed side effects included mild gastrointestinal discomfort and headache, but these were similar between the two active treatments, indicating no major safety concerns specific to IBA [77]. Similar results have been collected from another identical in terms of study design, objective, and patient population [78].
Another randomized, double-blind, placebo-controlled, cross-over trial aimed to compare IBA, with ibuprofen in terms of onset, peak effect, and overall analgesic efficacy in dysmenorrhea. The study included a total of 104 women with a history of moderate to severe primary dysmenorrhea and analyzed data over five consecutive menstrual cycles. Each participant received IBA (200 mg or 400 mg), ibuprofen (200 mg or 400 mg) or placebo. Study findings indicate that IBA 400 mg provides significantly faster pain relief compared to ibuprofen. Specifically, the median time to meaningful pain relief was 56 min for IBA 400 mg, whereas patients receiving ibuprofen reported meaningful relief only after 86–90 min (p < 0.05). Despite this difference in onset speed, both formulations achieved similar peak pain relief, suggesting that while IBA accelerates the onset of analgesia, it does not increase the overall intensity of pain relief beyond that provided by ibuprofen. Furthermore, the need for rescue medication was notably lower in both active treatment groups compared to placebo. All treatments demonstrated a favorable tolerability profile, with no statistically significant differences in the incidence of adverse events among the treatment groups. The most frequently reported AEs included headache, nausea, and dizziness, which occurred at comparable rates across IBA, ibuprofen, and placebo groups. Importantly, no serious adverse events were observed, and no patient discontinued the study due to treatment-related adverse effects, highlighting the safety and acceptability of both ibuprofen formulations in the management of dysmenorrhea [76].
The Use of IBA to Enhance Anesthetic EfficacyRecently, IBA has also been evaluated in enhancing anesthetic efficacy. Oliveira et al. [79] conducted a double-blind, randomized clinical trial to evaluate the preemptive administration of IBA (1155 mg) compared to ibuprofen (600 mg) and placebo in improving the anesthetic success of inferior alveolar nerve block (IANB) in patients with symptomatic irreversible pulpitis. A total of 150 participants were randomized into three groups, and success was determined as mild or no pain during treatment. The study found that IBA significantly increased IANB success rates (78%) compared to ibuprofen (62%) and placebo (34%) (p < 0.001). Additionally, preoperative anxiety and pain intensity influenced the block’s efficacy. Patients with successful blocks reported lower anxiety scores (median: 8) and lower preoperative pain scores (mean: 118.3) than those with failed blocks (anxiety median: 15, pain score mean: 132.1, p < 0.001 and p = 0.025, respectively) [79].
Comments (0)