Thyroid surgery is one of the most frequently performed surgeries with low mortality and varied morbidity. Although the rate of complications after thyroidectomy is low, complications such as postoperative bleeding, hypocalcemia, airway problems, vocal cord paralysis, infection, hemorrhage, and hematoma have been reported [19].
In the study, it was observed that the highest prevalence of thyroidectomy was in females (83.9%). Studies in the literature have shown that thyroidectomy surgery is performed similarly at a rate of 71–85%, primarily in women [20,21,22,23,24,25]. As evidenced by the study results, thyroidectomy prevalence is generally higher in females than males.
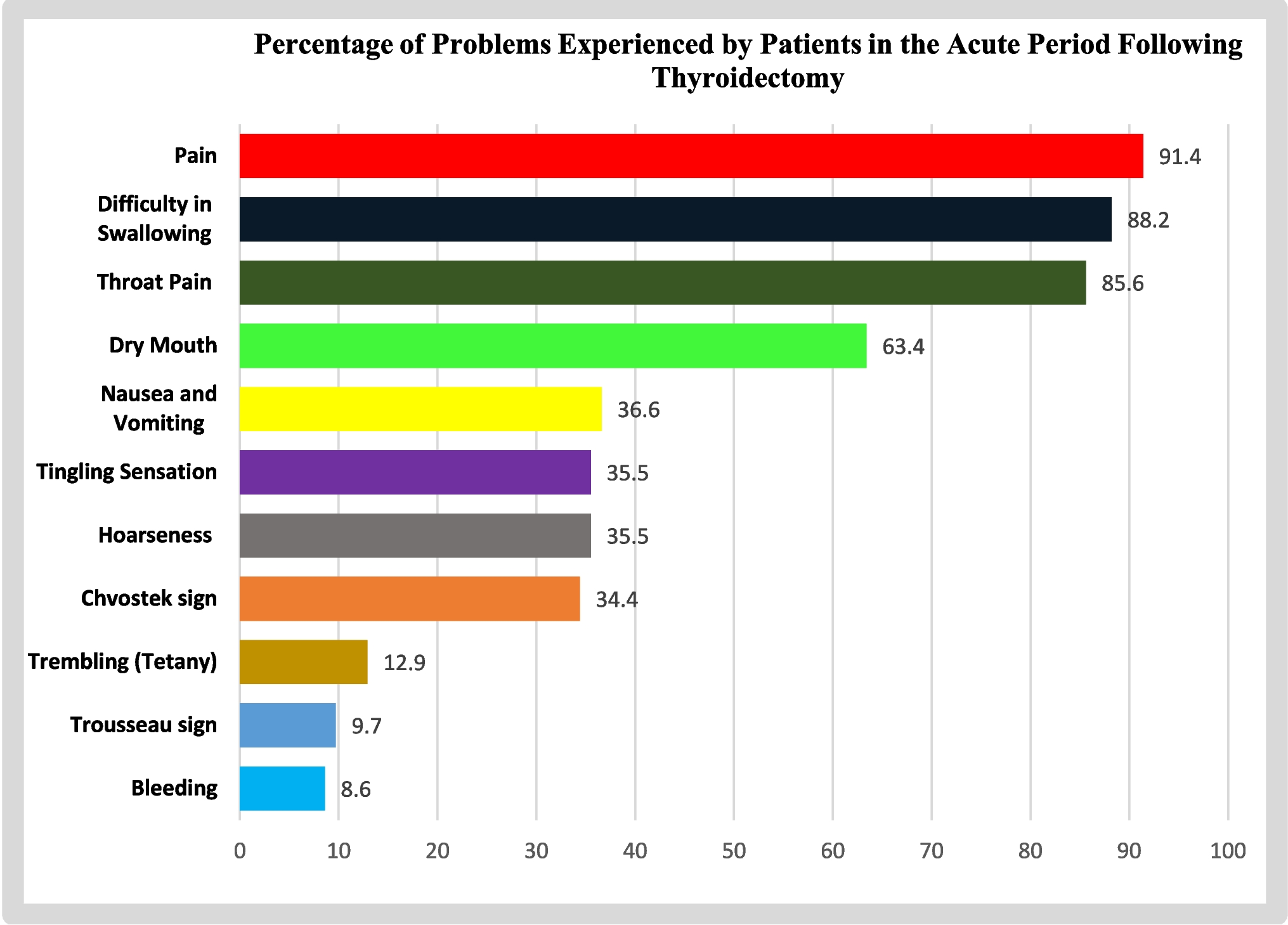
The study observed a significant decrease in the preoperative calcium level, with hypocalcemia detected in 24% of the patients. Chvostek’s sign was positive in 34.4% of the patients, and Trousseau’s was positive in 9.7%. Tingling was observed in 35.5% and tremors (tetany) in 12.9% due to low serum calcium levels. In the study, which evaluated early and late complications after thyroidectomy, hypocalcemia was determined to be the most common complication, with a rate of 54.4% [20]. Another study reported the mean postoperative calcium level as 9.31 mg/dl on the first day and 8.21 (4.8–9.9) on the second day [26]. Temporary hypocalcemia was detected in 28% of the patients included in the study. These findings underscore the prevalence and urgency of addressing hypocalcemia in postoperative care.
Statistical analysis revealed significant differences in factors affecting hypocalcemia, including female gender, preoperative diagnosis, intraoperative parathyroid damage, and small nodules with low vitamin D levels. In the study by Yabanoğlu et al. (2019) [23], transient hypocalcemia was detected in ten patients (6.8%) and permanent hypocalcemia in two patients (1.4%) after surgery. In a prospective study, hypoglycemia was observed in 70% of cases. No significant differences were observed in terms of demographic data, malignancy diagnosis, thyroid size, 25(OH)D status, previous treatment, and neck dissection with hypocalcemia. At the end of the study, it was stated that postoperative hypocalcemia remains the most common complication, and the process of prevention and treatment is still not adequately evaluated [26]. Although the percentage of hypocalcemia varies according to different parameters in the literature, it continues to be the most common problem after surgery.
When examining problems occurring within the first 24 h after surgery, it was found that patients experienced pain, difficulty swallowing, throat pain, dry mouth, nausea/vomiting, tingling and hoarseness, Chvostek’s sign, tremors (tetany), Trousseau’s sign, and bleeding. In studies investigating early and late complications after thyroidectomy, investigating early and late complications after thyroidectomy, hoarseness was observed in 33.3% of patients, difficulty swallowing in 32.8%, and hematoma formation in 0.53% of patients in another study [5, 20]. Kwon et al. reported no bleeding in any patients after thyroidectomy, while transient recurrent laryngeal nerve palsy occurred in 11.5% and permanent in 2.3% [27].
In the study by Reizian et al. (2023) [28] examining postoperative pain, all patients in the control group and 90% of patients in the intervention group experienced neck pain within the first 24 h. This was observed in 100% and 83.3% of patients before discharge. One week after surgery, neck pain was observed in 83.3% of the intervention group and most of the control group (90%). In another study examining pain, it was reported that the median pain score for patients was 5, with 53% of them transitioning to chronic pain [29]. In an experimental study investigating the effect of neck exercises on postoperative pain conducted by Türkmen et al. (2022) [30], the mean pain score on the first day after surgery was 2.20 ± 2.22 for the intervention group and 3.00 ± 2.10 for the control group, with no statistically significant difference found.
Before surgery, the average Richard Campbell Sleep Questionnaire (RCSQ) score for patients was 70.078, which decreased to 40.723 predischarge. A statistically significant difference was found between the post-thyroidectomy RCSQ scale averages and throat pain, difficulty swallowing, pain, Chvostek’s sign, and Trousseau’s sign (p < 0.05). However, no statistically significant difference was observed between postoperative RCSQ scale averages and hoarseness, dry mouth, nausea-vomiting, bleeding, tingling, and tremors (p > 0.05). In the study conducted by Koo et al. (2022) [13] evaluating the preoperative sleep quality of patients undergoing thyroidectomy surgery, it was found that 35 patients (76.1%) had poor preoperative sleep quality. Postoperatively, it was determined that PSQI scores at 1, 4, and 10 months were significantly lower compared to pre-operative scores (p < 0.001). Patients experienced sleep disturbances for at least 10 months before and after surgery. The PSQI scores over 5 years post-surgery were significantly decreased compared to pre-operative scores (p < 0.001).
La et al. (2117) [31] compared sleep quality in patients undergoing parathyroidectomy and thyroidectomy and found that parathyroid patients had worse pre-operative PSQI scores than thyroid patients. Before surgery, a more considerable proportion of parathyroid patients exhibited poor sleep quality (PSQI score > 5) compared to the thyroid group (69% vs. 51%). Another study observed that on the first day postoperatively, 40% of patients experienced sleep problems, 100% experienced pain, 95% experienced respiratory problems, 98.3% experienced eating and drinking issues, and 83.3% experienced communication problems. By the end of the first week, these percentages decreased to 3.3%, 28.3%, 13.3%, 18.3%, and 21.7%, respectively. Patients experienced problems up to 4 weeks postoperatively, indicating that they faced challenges, particularly on the first day and first week after surgery [32].







Comments (0)