
Remember me
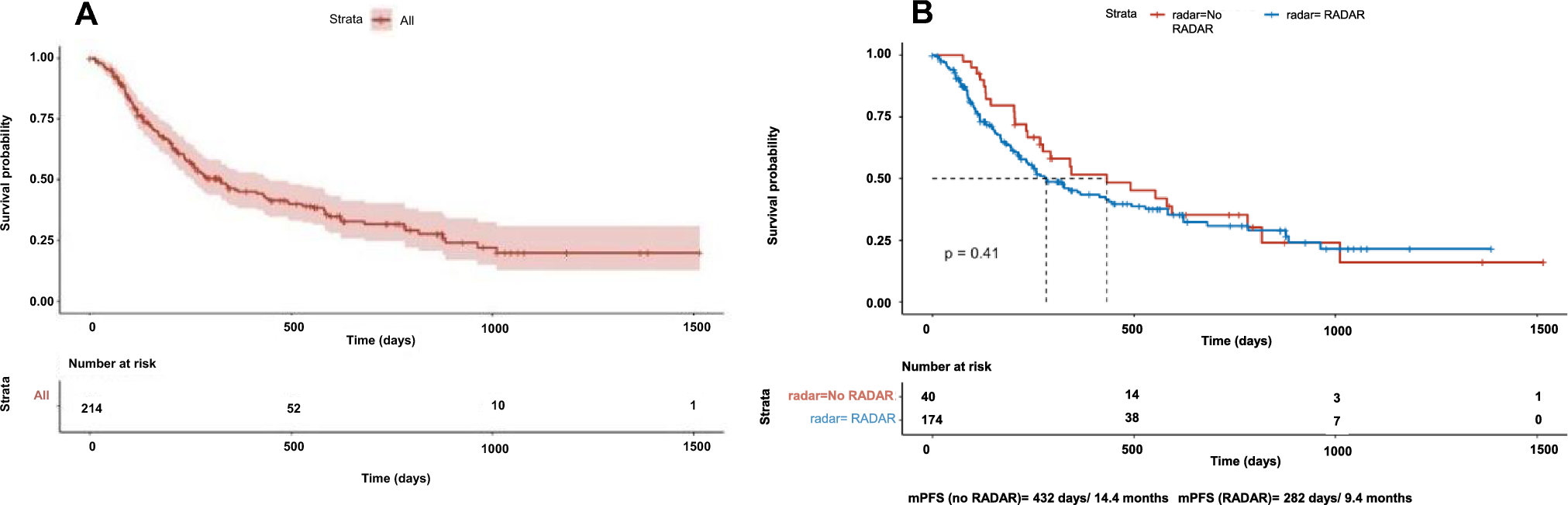





In this retrospective multicentric analysis done on a “real life” patient population, we showed that brigatinib has an inconstant efficacy in ROS1 patients. Nevertheless, it appears that some heavily pretreated patients can derive prolonged benefit from the drug. Despite a limited number of patients, our study represents the largest cohort in the setting of this rare population of pretreated ROS1 patients.
The mPFS of our study is 3.8 months, however, with a wide gap between patients, ranging from 2 months to more than 5 years. This could be explained on one hand by the compassionate access of our study, with “real life” patients, the majority of them being treated with multiples lines of treatment with an increased risk of intrinsic tumoral resistance.
Few studies have reported the use of brigatinib in patients who have progressed following crizotinib treatment. One retrospective study evaluating seven patients with crizotinib-resistant ROS1 NSCLC reported an ORR of 29%, for a disease control rate of 43%. PFS was not evaluable [19].
In a phase II multicentric basket study, called the Barossa cohort, brigatinib was used in three patient cohorts with a ROS1-positive tumor. In 19 crizotinib-resistant ROS1 NSCLC patients, the ORR was 31.6%, with a disease control rate of 57.9%. The mPFS was 7.3 months in this population [20], which is higher than our study, but patients had only received crizotinib, whereas in our population, some patients were heavily pretreated with more options than crizotinib only.
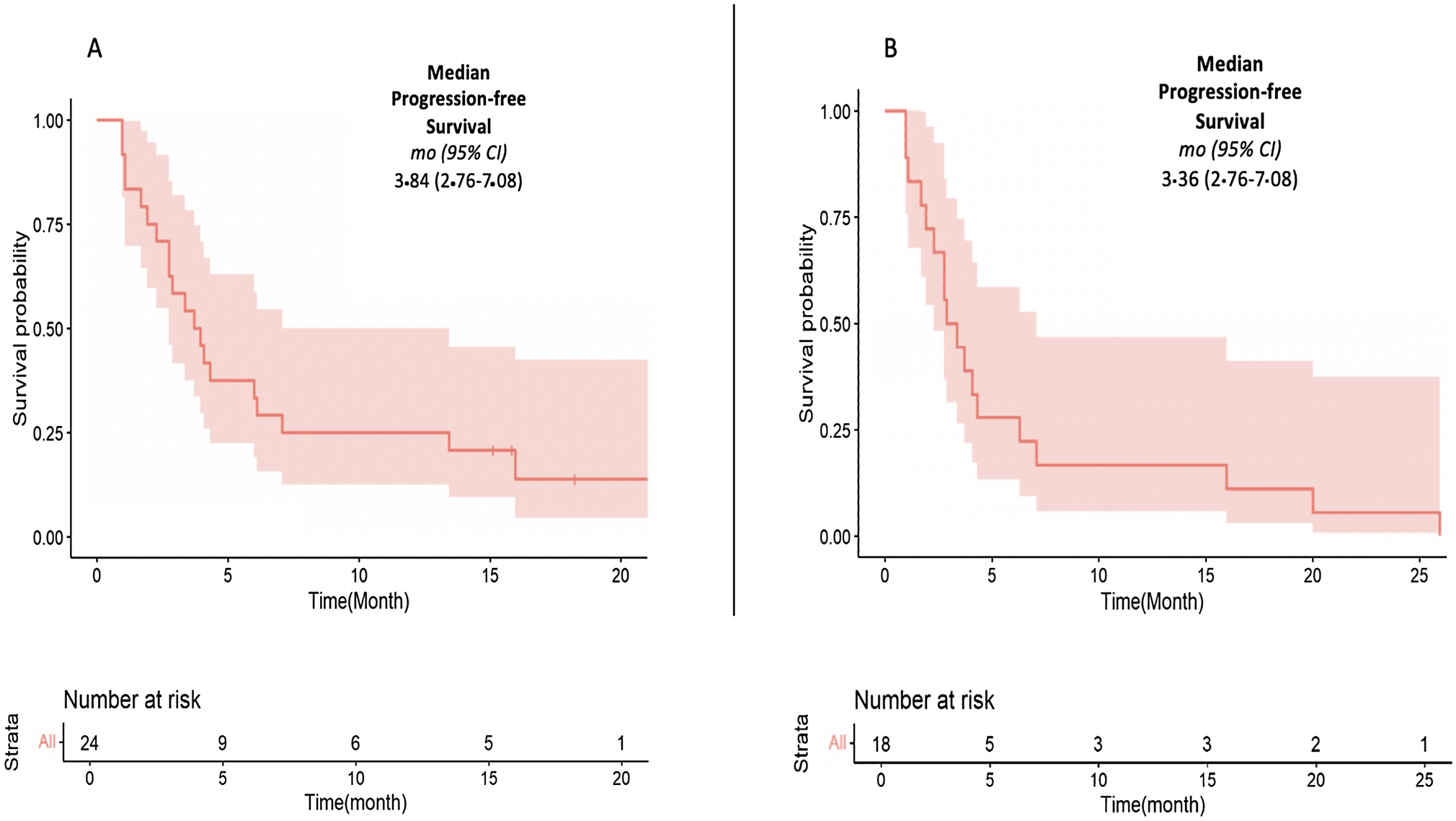
These two studies compared with our study are shown in Fig. 3.
Fig. 3
Comparison of the three largest series performed in patients with ROS1 metastatic NSCLC under treatment with brigatinib who had crizotinib resistance. NSCLC non-small-cell lung cancer, ORR objective response rate, PFS progression-free survival
Other therapeutic options in ROS1-rearranged NSCLC have been tested. Ceritinib showed an ORR of 62%, and mPFS was 9.3 months for all patients and 19.3 months for crizotinib-naïve patients in a multicentric phase II study [10]. Entrectinib, a neurotrophic tyrosine receptor kinase (NTRK) inhibitor, active on ROS1, was associated with a 77% ORR and a median duration of response of 24.6 months in a pooled-analysis on 56 patients [11]. Repotrectinib is also an NTRK and ROS1 inhibitor; it demonstrated potent activity, with an ORR of 79% and an mPFS of 35.7 months [12]. Finally, lorlatinib showed an interesting ORR of 62% and an mPFS of 21 months in TKI-naïve patients. Following crizotinib resistance, lorlatinib is a preferred option due to its central nervous system diffusion, with an ORR of 35% and an mPFS of 8.5 months [13].
ROS1 therapeutic resistance mechanisms are insufficiently analyzed in practice. Only one rebiopsy following brigatinib resistance was performed in our study, and found a G2032R resistance mutation, conferring potential resistance to this treatment. These mutations were probably not investigated enough in this study, as systematic biopsies were not mandatory.
Few serious side effects were reported in our study, supporting the favorable safety profile of brigatinib, which is concordant with preexisting data. However, this study did not include the systematic collection on all side effects with brigatinib, such as diarrhea or asthenia.
The only grade 3 side effect was a dilated heart disease, potentially imputable to brigatinib, although the medical literature does not report this type of severe side effect.
Our study shows some limitations. The retrospective pattern of this study and the limited number of patients are one known limitation, however well described and inherent to the ROS1 population in NSCLC. Another important limit lies in the compassionate access to brigatinib, which initially specified pretreatment with at least two prior ROS1-targeted therapies and a chemotherapy. However, some patients received brigatinib outside these recommendations, with only one prior line of treatment with crizotinib. In these eight patients, only three patients presented with a partial response and the others did not show any response. This seems consistent with the ORR and disease control rate of the global population.
Comments (0)