
Remember me








After we had started to use IGABT, between May 2012 and April 2024, 183 patients suffering from histologically proven cervical cancer and not suitable for surgery underwent radical radiotherapy (RT) or CCRT at the Department of Oncology and Radiotherapy, University Hospital Pilsen, Czech Republic. Of this cohort, we analysed only patients who underwent pretreatment staging, subsequent mid-treatment evaluation after completed EBRT and definitive restaging 3 months after completing the whole treatment, in each case using PET/MRI. A total of 108 patients met these criteria, all of whom were treated at our department between August 2015 and January 2023. In the period preceding August 2015, we had used only MRI or PET/CT, as PET/MRI was not yet available in our hospital.
The median age of the analysed patients was 57 years (range 32–83 years). Almost half of the patients (48; 44.5%) had been diagnosed at stage IIIC1 according to the 2018 International Federation of Gynecology and Obstetrics (FIGO) classification [8]. Thirty patients (27.8%) were diagnosed at stage IIB, 22 patients (20.4%) at stage IIIC2 and 5 patients (4.6%) at stage IVB. One patient (0.9%) each had stage IB1, IIIB and IVA (Table 1). All patients signed an informed consent form prior to any treatment modality and any imaging procedure.
Table 1 Patient, tumour and treatment characteristics. The medium age of the patients was 57 (range 32–83)External-beam radiotherapy and brachytherapy planning, chemotherapyIn all 108 patients (100%), EBRT was combined with brachytherapy (BT). All patients underwent pretreatment staging with PET/MRI before RT or CCRT was initiated. EBRT planning was based on a contrast-enhanced CT scan of the abdomen and pelvis of patients in a supine position. Treatment planning as well as the treatment itself were performed with full bladder and empty rectum. We used either intensity-modulated radiotherapy/volumetric modulated arc therapy (IMRT/VMAT; 33 patients, 30.5%) or IMRT/VMAT with a simultaneous integrated boost (IMRT/VMAT-SIB; 75 patients, 69.4%). All patients were treated with pelvic EBRT. Patients received extended-field RT that included the paraaortic lymph node regions if lymph node involvement in either the paraaortic or pelvic nodal chains had been confirmed. The prescribed dose of EBRT was 45 Gy. In the presence of lymphadenopathy, the IMRT/VMAT-SIB technique was used with two dose levels of 45 Gy or 55 Gy in 25 fractions. Lymphadenopathy was not confirmed by biopsy in any patient. Two patients had small nodal involvement in the lower mediastinum (and this area was part of the target volume), and one patient each had metastases in the left supraclavicular area (which regressed after ChT), right ovary (part of the target volume) and rectovaginal septum (also part of the target volume). The IMRT and the VMAT plans were normalized to cover ≥ 99% of the planning target volume (PTV) with 90% of the prescription dose and ≥ 95% of the PTV with 100% of the prescription dose. Plans were optimized in the Monaco® treatment planning system (Elekta, Stockholm, Sweden). All sets of plans were created using the same 10-MV photon beams from an Elekta Synergy linear accelerator equipped with an 80-leaf multileaf collimator. Patients were treated using either IMRT plans with nine coplanar fields using equally spaced gantry angles or with VMAT plans, which were performed using two coplanar arcs.
In 93 cases (86.1%), EBRT was combined with concomitantly administered chemotherapy (ChT) with cisplatin 40 mg/m2 weekly (Table 1). However, most patients did not receive all possible cycles of chemotherapy, mainly due to haematological toxicity and incipient renal insufficiency.
Immediately after the end of EBRT, BT was applied with a total of four planned applications. In all patients, we applied 3 T-MRI-based image-guided adaptive BT (IGABT) with the uterovaginal applicators Vienna Ring CT/MR, Interstitial Ring CT/MR or Venezia applicator (Elekta); the treatment planning systems Oncentra Masterplan® and Oncentra Brachy® (Elekta); and HDR (high-dose-rate) after-loading machines MicroSelectron® and Flexitron® (Elekta) with an iridium (192Ir) source. The whole procedure and treatment planning were performed according to the recommendations issued by the Gynaecological Working Group of the Groupe Européen de Curiethérapie (GEC) and the European Society for Radiotherapy and Oncology (GEC-ESTRO) published in 2005 and 2006 [9, 10] and also adopted by the American Brachytherapy Society (ABS) [11, 12]. The prescribed dose was 7 Gy to the 100% isodose. The coverage goal was quantitatively evaluated by the high-risk clinical target volume (HR-CTV) D90 (the dose covering 90% of the HR-CTV), which should ideally exceed 100% of the prescription dose. All doses were reported as the equivalent dose corresponding to the conventional fractionation using 2 Gy per fraction (EQD2). The linear quadratic model with values of α/β = 10 for the tumour and α/β = 3 for organs at risk was used for the dose recalculations, as described in detail in our previous publication regarding clinical outcomes and late side effects of 3D BT in cervical cancer in our institution [13, 14].
PET/MRI protocolThe PET/MRI scans were obtained using an integrated PET/MRI scanner (Biograph mMR, Siemens Healthineers, Erlangen, Germany). Patients were advised to abstain from food for a duration of 6 h, and their blood glucose levels were measured to verify values below 150 mg/dL. Eligible patients received the radiopharmaceutical 18F-FDG with an activity of 2.5 mBq/kg. Following a 60-minute accumulation interval, PET images and MRI data were simultaneously acquired.
In the initial phase, a comprehensive diagnostic MRI examination of the pelvis was performed. The MRI protocol included T2-weighted high-resolution images in transversal and sagittal projections, diffusion-weighted images (b values 50 and 800), and T1-weighted images in transverse projection before and after the administration of a gadolinium-based contrast agent (4 ml of gadobutrol). Dynamic acquisition of T1-weighted sequences was also performed. Additionally, FDG uptake in the pelvis was obtained simultaneously within 15–20 min.
This was followed by a whole-body MRI examination using the Dixon volumetric interpolated breath-hold examination (VIBE) T1-weighted sequence method useful for calculating the attenuation correction of PET images. Four datasets of T1-weighted images were reconstructed for analysis. The acquisition time in each position was up to 4 min, and the PET acquisition was adjusted to match the MRI sequence’s total duration for that specific position.
Image analysisUsing dedicated software (MM Oncology, SyngoVia; Siemens Healthineers), two radiologists experienced in hybrid imaging independently performed image analysis, and the measured values from both were averaged. MRI images were used to record three orthogonal distances of the cervical tumour (tumour size), followed by semiautomatic segmentation of the corresponding FDG lesion. Additional recorded parameters included SUVmax (maximum standard uptake value), SUVpeak (average SUV within a small, fixed-size region of interest [ROI] centred on a high-uptake region of the tumour), SUVmean (mean SUV value) and MTV (metabolic tumour volume). Total lesion glycolysis (TLG; TLG = MTV × SUVmean) was also calculated. A similar procedure was used to assess lymph nodes, whereby lymph nodes with SUVmax > 2.5 were considered metastases.
In addition, we also recorded the sum of the MTV of the primary tumour and pelvic and para-aortic lymph nodes (MTV-S) as well as the sum of TLG for the primary tumour and pelvic and para-aortic lymph nodes (TLG-S). Pretreatment parameters (pre-SUVmax, pre-SUVpeak, pre-SUVmean, pre-MTV, pre-MTV‑S, pre-TLG and pre-TLG-S) and treatment-specific parameters at week 5 (mid-SUVmax, mid-SUVmean, mid-SUVpeak, mid-MTV, mid-MTV‑S, mid-TLG and mid-TLG-S) were recorded. To measure the apparent diffusion coefficient (ADC), an ROI was manually placed within the region with the highest FDG uptake and maximal area, avoiding surrounding tissues.
Furthermore, we recorded absolute and relative (percentage) changes in all investigated parameters between pre- and mid-PET/MRI (∆ and ∆%), except for SUVmean and SUVpeak.
Treatment response evaluationThe response to treatment evaluated by mid-PET/MRI (typically performed at week 5) was categorized into three types based on the RECIST 1.1 [16] and PERCIST [17] criteria:
1.Interim complete metabolic response (ICMR): No morphological or metabolic evidence of cancer on mid-PET/MRI, regardless of initial staging (Fig. 1).
2.Interim nodal response (INR): Absence of morphological and metabolic signs of nodal involvement and incomplete local remission, regardless of initial staging.
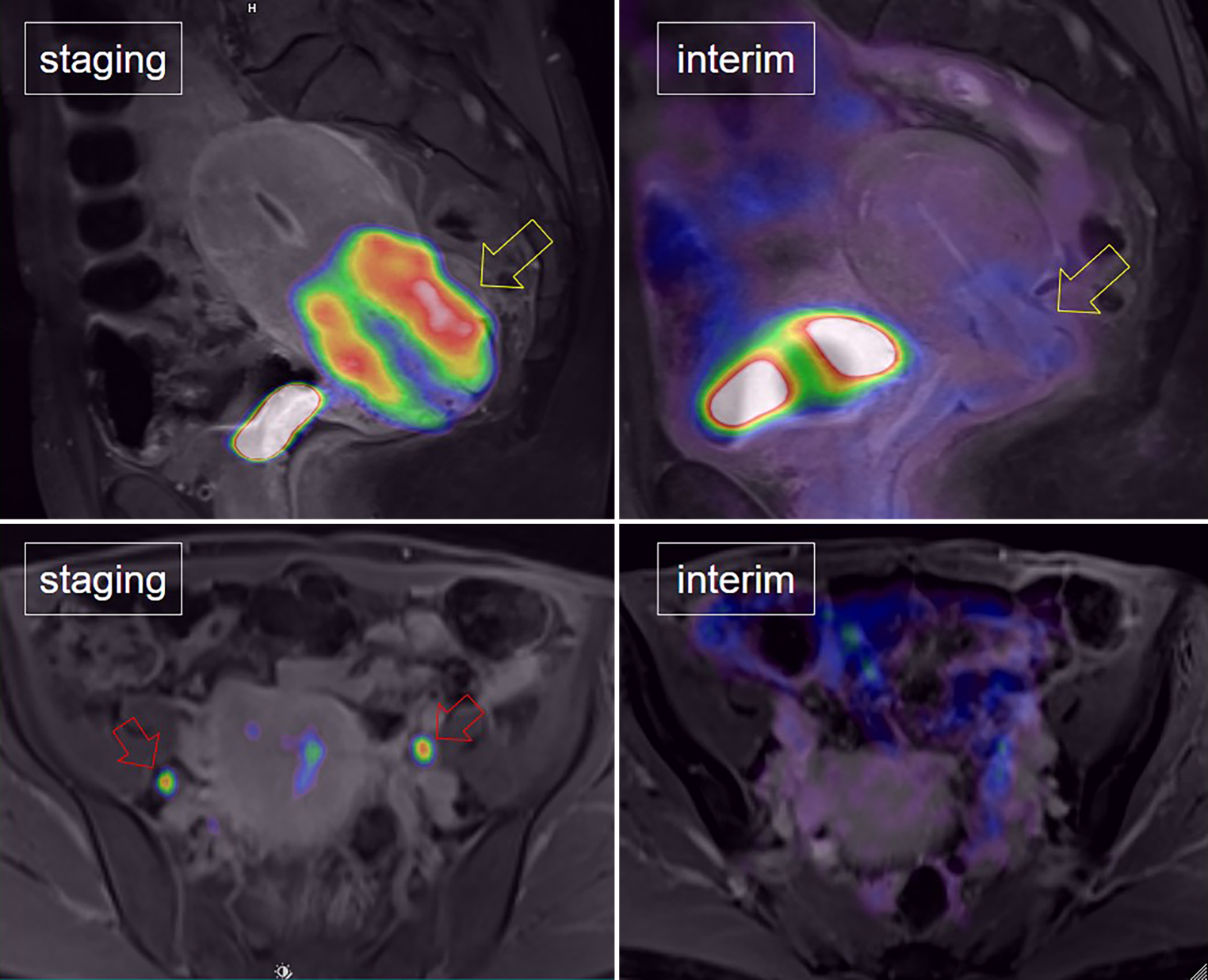
3.Interim nodal persistence (INP): Persistent morphological or metabolic signs of nodal involvement after initial N1 or N2 findings and incomplete local remission (Fig. 2).
Fig. 1
In a patient with cervical cancer, a complete metabolic response was observed. This was characterized by the complete disappearance of FDG uptake in both the primary cervical cancer lesion (yellow arrow) and the bilateral pelvic lymph node metastases (red arrows)
Fig. 2
In a patient with cervical cancer, an incomplete metabolic response was observed. This was characterized by the persistence of FDG uptake in both the primary cervical cancer lesion (yellow arrow) and the bilateral pelvic lymph node metastases (red arrows)
The combination of persistent nodal involvement and complete local remission at interim evaluation was not observed in the overall cohort.
Patients were then divided into two groups based on RECIST 1.1 and PERCIST criteria: those who achieved a complete metabolic response (CMR) and those who did not. CMR was defined as the absence of metabolically active lesions on post-PET/MRI performed 3 months after treatment, while any other finding was classified as non-CMR. These two groups were compared using metabolic, functional and morphological parameters obtained at pre-PET/MRI and mid-PET/MRI as well as using the absolute and relative changes in these parameters between the two examinations.
To evaluate correlations between the parameters of interest and survival outcomes, we used disease-free (DFS) and overall survival (OS). Local control (LC) was excluded due to only four cases of local recurrence in the entire cohort, thus rendering the results uninformative. DFS was defined as the period between treatment commencement and any relapse or death (both regarded as complete observations). Patients without relapse at the end of follow-up were censored. OS was defined as the duration from treatment initiation to death, with surviving patients censored at the last follow-up date.
In addition to the post-PET/MRI examination, our department conducts comprehensive gynaecological examinations, including pelvic ultrasound, at regular intervals of 3 to 6 months. Further investigations are only necessary if patients exhibit symptoms and there is substantial suspicion of disease recurrence.
Statistical analysesStandard frequency tables and descriptive statistics were used to characterize the patient sample. Because of significantly nonnormal distributions of most of the recorded variables, the differences between responders and nonresponders were tested for statistical significance using the Mann–Whitney U test.
The prediction potential of the recorded variables with respect to non-CMR was assessed using the receiver operating characteristic (ROC). The ROC curve, describing the observed sensitivity and specificity values across all possible threshold values within the range of a particular variable, was plotted for each variable. The area under the curve (AUC ROC) was then calculated to summarize the prediction factor in a single value, ranging from 1 (perfectly reliable prediction) to 0.5 (random guessing). Sensitivity and specificity were determined for specific threshold values. To assess the potential confounding of these predictors by TNM variables, the ROC analysis was repeated on a subsample uniform in terms of T and M (T2M0; 87 patients) in which the predictor values were also adjusted for the effect of N (i.e. divided by the mean value of the appropriate N category and then multiplied by the whole-sample mean).
Median follow-up time was determined using the inverse Kaplan–Meier method. The Kaplan–Meier survival curve estimation method along with the Gehan–Wilcoxon significance test was used to assess the associations of survival with categorical variables. The Cox proportional hazards model was used to explore the associations of continuous variables with survival. In order to visualise these associations with Kaplan–Meier plots, threshold values were determined for the continuous prognostic variables using an automated process. In this process, the Cox–Mantel p-values achieved after stratification of the sample into two groups by a particular continuous variable were calculated and plotted against all possible threshold values within the range of the variable, with a minimum group size of 10. Subsequently, the plots of p-value against threshold value were examined and a threshold value with good performance for both OS and DFS was determined for each continuous prognostic variable. In order to verify the independence of the prognostic variables, a multifactorial categorical Cox model was created for each of the major stratified predictors together with TNM factors and age.
All reported p-values are two tailed, and the level of statistical significance was set at α = 0.05. The STATISTICA data analysis software system (version 12; StatSoft, Inc. 2013. Tulsa, OK, US) was used; the ROC analysis, Cox proportional hazards model and threshold determination for survival predictors were implemented in MATLAB (released 2019a, The MathWorks, Inc., Natick, MA, USA).
Comments (0)