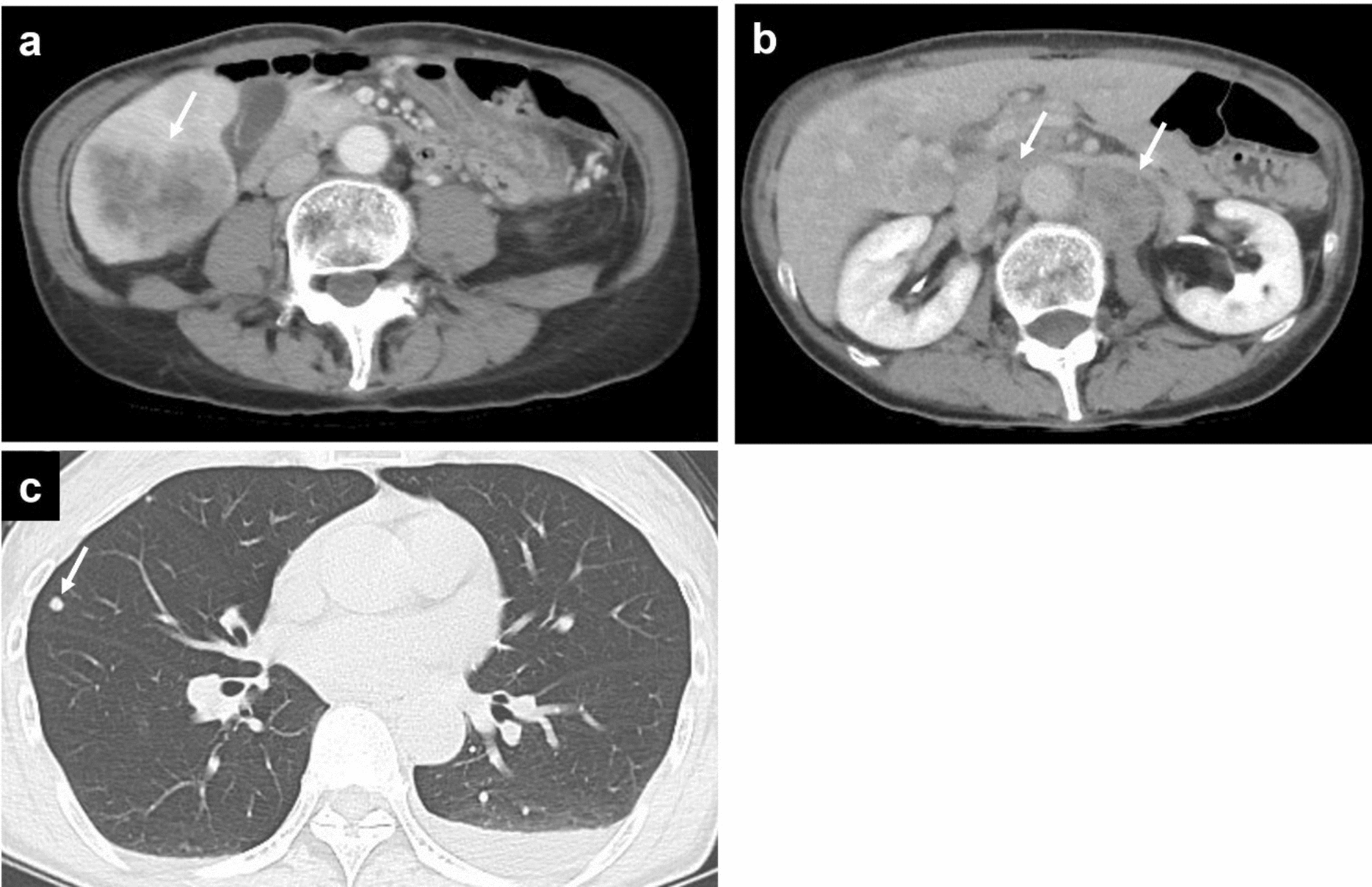
In this case, the patient underwent surgical resection of the lesion after being diagnosed as an SMT of the ascending colon. SMTs are lesions that originate below the submucosal layer, often protruding into the gastrointestinal lumen and covered with non-neoplastic mucosa. These tumors include lipomas, carcinoids, lymphangiomas, GISTs, and malignant lymphomas. SMTs with calcification, as observed in the present case, include GISTs, liposarcomas, and rectal carcinoid tumors [3, 4]. In large GISTs, localized calcification is common and often appears circumscribed, mottled, or patchy [5]. Extensive calcification throughout most parts of the tumor has seldom been reported [6,7,8]. In this case, although rare, a GIST with calcifications was suspected based on similarities with the imaging features of previously reported cases.
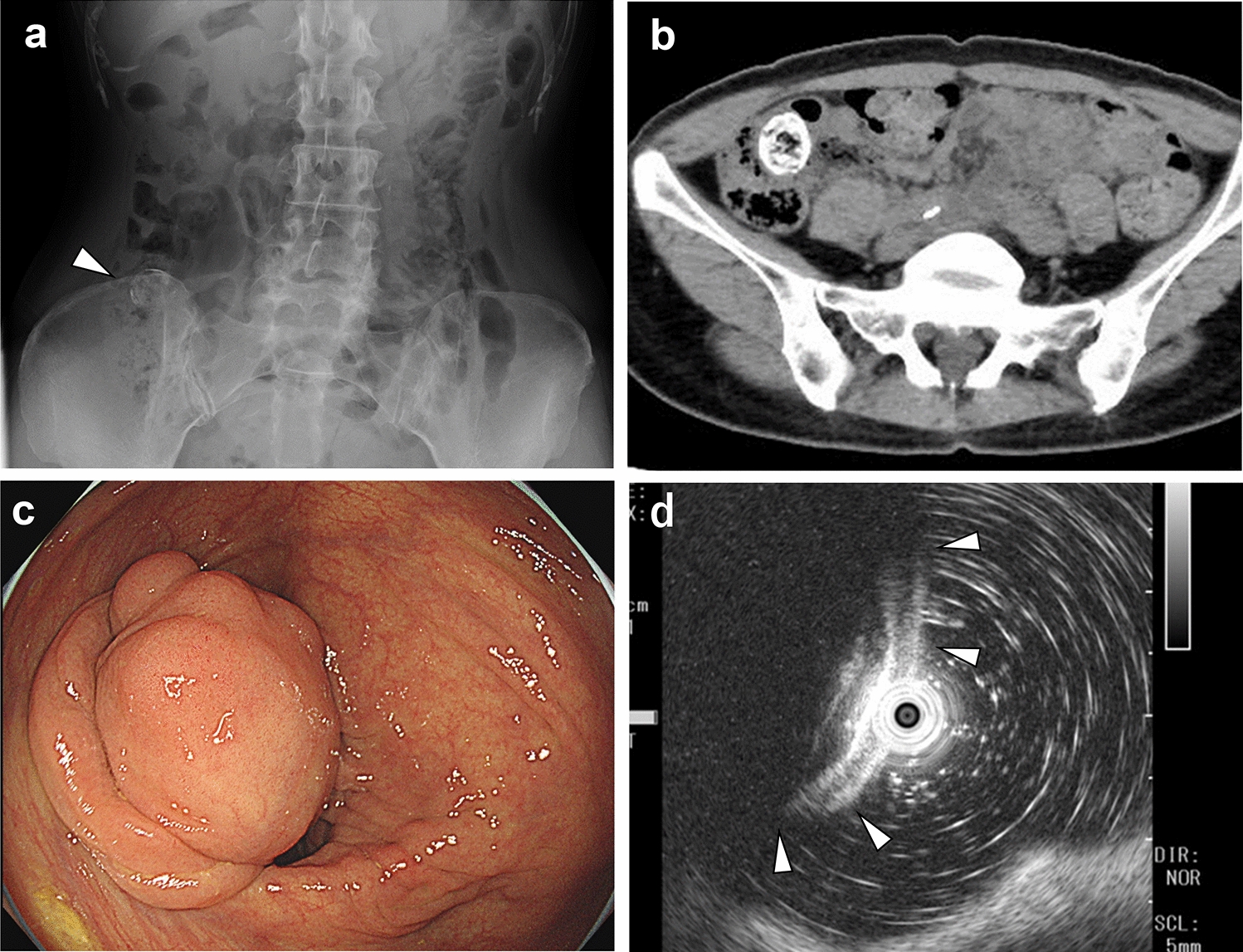
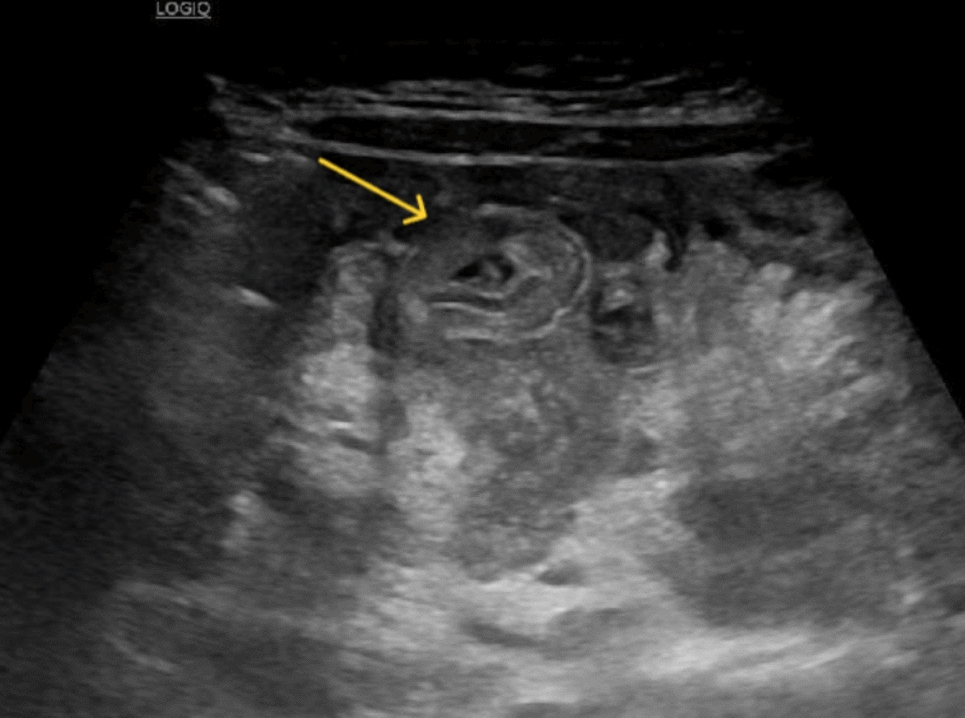
An inverted colonic diverticulum (ICD) is a diverticular lesion protruding into the intestinal lumen. It is observed in approximately 1.7% of patients on endoscopic examinations and has a polyp-like appearance [9]. Reverting the lesion to its normal position using forceps or insufflation is diagnostic in such cases [10, 11]. Additionally, the concentric circle pattern of colonic mucosa, which becomes more evident with narrow-band imaging [12], aids the diagnosis of diverticulosis [9]. Caution is required because a biopsy or polypectomy for ICD may result in perforation. In this case, while the diverticulum protruding into the lumen resembled an inverted diverticulum, it was not an inversion but an expansion of the diverticulum toward the lumen, indicating a different pathology. In addition, colonic diverticula are often pseudodiverticula; however, in our case, the patient had a diverticulum with all layers of the colonic wall.
Inada et al. presented a rare case of a pedunculated, feces-filled, non-inverted pseudodiverticulum in the ileum [13]. Based on the lack of ectopic tissue, a muscular layer, and feces inside the diverticulum, the authors concluded that the lesion was different from an inverted diverticulum. According to the authors, such lesions rarely occur in the colon, presumably because the orifice of the colonic diverticulum is usually large enough for feces to return to the colon, and the extensibility of the colon is lower than that of the ileum. Therefore, colonic diverticula filled with feces merely enlarge and do not extend toward the lumen. We partially disagree with this hypothesis because the orifice of the diverticulum was large in our patient. Instead, we claim that the enlargement of the diverticulum is due to a balance between the extensibility and components of the colonic wall, the size of the orifice, and the viscosity of the feces. Although neither hypothesis can be further proven, we believe that our case is extremely rare. A PubMed search with the keywords “diverticulosis,” “submucosal tumor,” and “colon” did not show any similar cases. Therefore, we consider this the first reported case of a large, non-inverted true diverticulum resembling an SMT.
Intestinal duplication is a possible differential diagnosis of the present case. It has been described clinically and pathologically by Ladd and has three characteristics: (1) well-formed smooth muscle layers, (2) an epithelial lining consisting of some portion of the alimentary tract, and (3) contiguity with a portion of the alimentary tract [14]. Although the present case has these pathological features, we diagnosed a true diverticulum rather than intestinal duplication based on the following points. First, most cases of intestinal duplications are observed before the age of 2 years, and this condition is rarely observed in adults [15, 16]. Ectopic gastrointestinal epithelium is often present in intestinal duplication; however, in the present case, there was no ectopic pancreas or gastric mucosa [16]. Intestinal duplication is classified as cystic or tubular according to its shape, and the cystic lesion usually does not have communication with the normal lumen [14, 16, 17]. In the present case, the lesion is cystic in shape but has communication through a large hole with the intestinal tract. Further, the muscular layer of the wall that formed the base of the diverticulum in the present case was thin compared to the other part of the colon, which we believe is supporting evidence that the case is a diverticulum. Meanwhile, Choong et al. explained that type 2 Giant Colonic Diverticulum is a true diverticulum and considered that its origin is most likely a duplication of the intestinal tract [18]. The difference between the two entities should be discussed further.
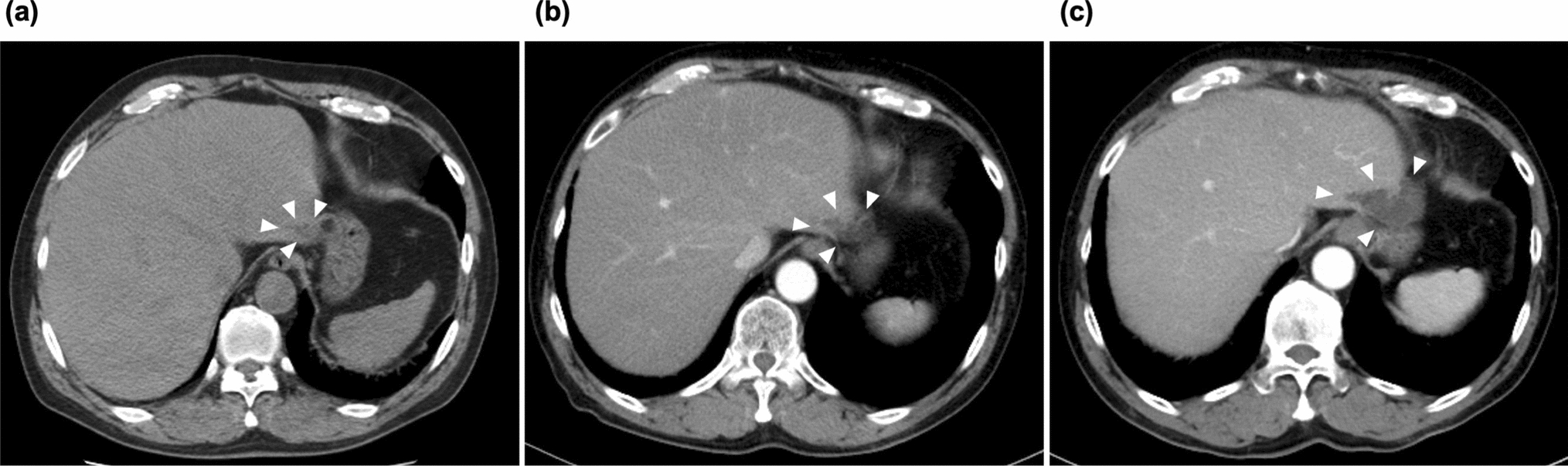
In this case, several factors contributed to the difficulty in making a definitive diagnosis. First, this condition is rare, and we encountered such a case for the first time, making it practically impossible to recall this condition. Second, colonic diverticula typically present as multiple lesions; however, in this case, the preoperative CT images and the excised specimen revealed only a single lesion. Third, the orifice of the diverticulum was located on the proximal side of the colon, making it challenging to locate the orifice during endoscopic examination.
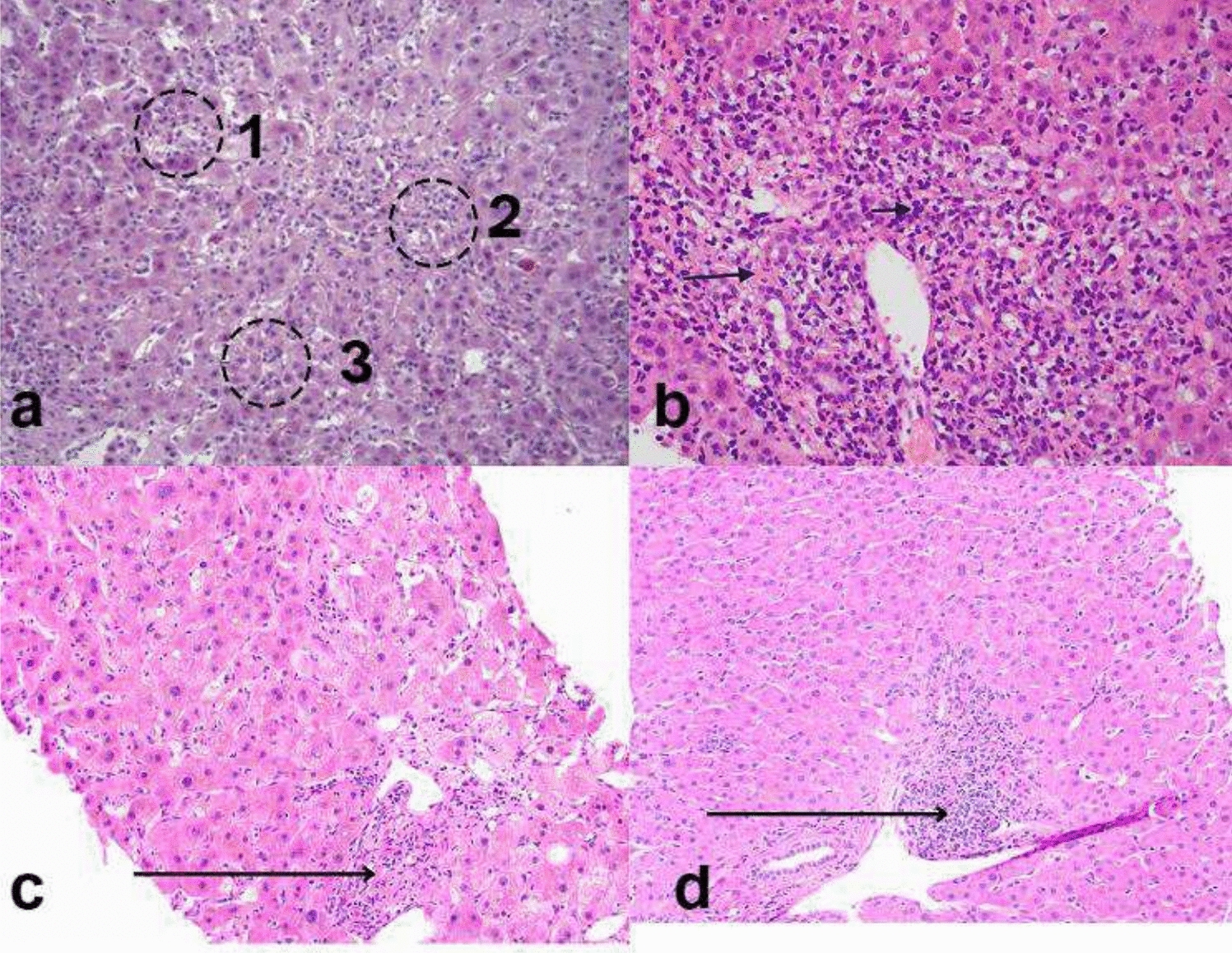
In the present case, her abdominal pain triggered the identification and treatment of the lesion. Pathologically, lymphocytic infiltration in the mucosal intrinsic layer and the submucosal layer was demonstrated, which may have been related to abdominal pain. Meanwhile, the protruded true diverticulum might have been tractioned toward the lumen. The pain might have been caused by such traction and the obstruction of outflow at the end of the ileum. Although surgery is often chosen for symptomatic tumors, if a colonic true diverticulum is accurately diagnosed and there are no symptoms, observation may be an option. In this regard, this case is worth reporting and true diverticulum should be included in the differential diagnosis of submucosal tumors with calcification.
We present a rare case of a colonic diverticulum filled with fecal matter that was difficult to distinguish preoperatively from an SMT. As the treatment differs, this entity should be included in the differential diagnosis of SMTs to ensure appropriate patient management.


Comments (0)