We present a rare case of metastatic thymoma that manifested with recurrence of gastrointestinal symptoms and severe malnutrition from intestinal failure attributable to thymoma-associated autoimmune disease. Our case highlights the heterogenous nature of thymoma manifestations, as the patient initially presented with myasthenia gravis, pure red cell aplasia and TAIE and had a recurrence of TAIE subsequently as a manifestation of metastatic disease. To the best of our knowledge, this is the first reported case of TAIE relapse due to thymoma recurrence. The diagnosis and treatment challenges of TAIE are discussed herein.
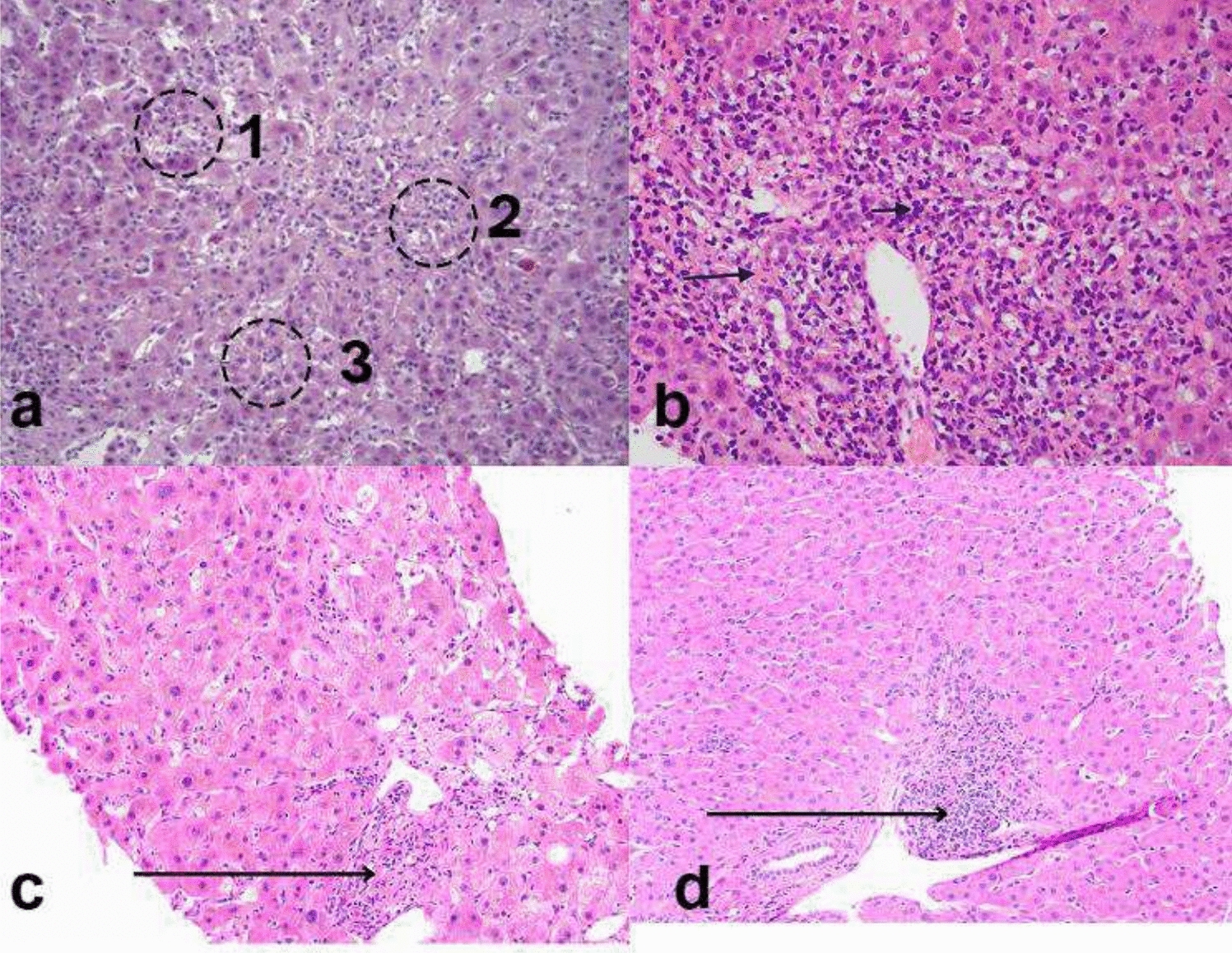
AIE as a cause of intractable diarrhoea is an important but rarely encountered differential diagnosis. Our patient’s history of previous thymoma and previous TAIE raised the clinical suspicion of relapsed disease, which was later confirmed by histopathological findings. She met the proposed diagnostic criteria for AIE: (a) chronic diarrhoea, (b) malabsorption, (c) specific small bowel histology of villous atrophy with the absence of goblet and Paneth cells, deep crypt lymphocytosis, increased crypt apoptotic bodies and minimal intra-epithelial lymphocytosis (Fig. 4), and (d) exclusion of other causes of villous atrophy. These histopathological changes typically affect the entire intestinal tract in AIE, which was confirmed by biopsies of the stomach and colon in our patient [11]. The widespread distribution of histologic findings excludes a differential diagnosis of coeliac disease, which is limited to the small bowel. Anti-enterocyte or anti-goblet cell antibodies were not tested in our case, but their absence does not exclude the diagnosis of AIE. Our patient had no dermatologic findings, as well as preserved immunoglobulin levels, arguing against a diagnosis of Good’s syndrome or TAMA. In addition, to our knowledge, there have been no descriptions of SSRI-related enterocolitis in the literature. SSRIs are a recognised cause of microscopic colitis, and while the colonic biopsies did contain increased intraepithelial lymphocytes that can be seen in microscopic colitis, the presence of conspicuous apoptotic bodies, complete absence of goblet cells and similar findings in the stomach and small bowel, are not features of that diagnosis. The initial clinical improvement in symptoms at index diagnosis despite continued SSRI intake, as well as the fact that there was no change in her dose when her symptoms recurred, again goes against a medication-related cause of enterocolitis. Finally, even in the presence of clinically significant diarrhoea and malnutrition associated with AIE, cross-sectional imaging is often unremarkable, as occurred in our case, with only up to 40% of cases having prominent mesenteric lymph nodes as their only radiological finding [12]. It is also important to note that the paucity of intra-abdominal fat, as well as the lack of luminal distension due to the absence of oral contrast in our patient’s CT modality, would have limited the assessment of the gastrointestinal tract.
There are no established guidelines for the treatment of TAIE, however, there are several case studies that report success in AIE with the use of corticosteroids (either prednisone or budesonide) [11, 13]. Unfortunately, up to two-thirds of these patients who achieve remission will become steroid-dependent or refractory [11]. Budesonide was chosen in our case given its high first-pass metabolism and reduced side effect profile. Mesalazine, which acts locally on colonic mucosa, was used as an adjunct. Although 5-aminosalicylate drugs have not been described as treatment for this condition, it was thought to be worth trialling as it is a low-risk drug with proven benefits in other autoimmune gastrointestinal diseases (namely ulcerative colitis). Unfortunately, the combined use of budesonide and Mesalazine in our patient did not induce histological remission by four months. Other agents including azathioprine, 6-mercaptopurine, cyclosporin, tacrolimus, mycophenolate mofetil, sirolimus, infliximab, rituximab and vedolizumab have shown variable success rates in the treatment of AIE [11, 14–19]. Given our patient’s history of metastatic thymoma and severe malnutrition that would render her at high risk of infection, as well as the unknown effects of strong immunosuppression on tumour progression, we were not inclined to pursue this therapy.
Intestinal failure is defined as “the reduction of gut function below the minimum necessary for the absorption of macronutrients and/or water and electrolytes, such that intravenous supplementation is required to maintain health and/or growth” [20]. Home parenteral nutrition, the treatment of choice for patients with intestinal failure, was recommended for our patient due to persistent malnutrition despite an adequate trial of oral and enteral nutrition. The patient’s informed decision to reject the utilisation of home parenteral nutrition to treat malnutrition was a major contributor to her clinical deterioration and subsequent death. Therefore, early recognition and reversal of malnutrition is a vital aspect of disease treatment.
Our patient had biopsy-proven autoimmune pangastritis, in the setting of anti-gastric parietal cell and intrinsic factor antibodies. This differs from the few cases of thymoma-associated autoimmune gastritis in the literature that have all occurred in the absence of autoantibodies [21, 22]. There are a few key factors in our case which clearly indicate that it is not an uncomplicated conventional autoimmune gastritis (AIG) despite having AIG autoantibodies: (1) involvement not limited to the corpus despite anti-gastric parietal cell antibodies, and (2) an absence of neuroendocrine cell hyperplasia and intestinal metaplasia. Therefore, it is difficult to ascertain whether the gastric involvement represents dual pathology of usual AIG and AIE, or part of the thymoma-related process.
The long-term outcome of patients with gastrointestinal autoimmune manifestations in the setting of metastatic thymoma is scarce. While surgical and/or chemotherapy options exist for metastatic thymoma, with a relatively good prognosis (38% 5-year relative survival rate), the safety and durability of treatment options may be limited by the emergence and complications of autoimmune diseases, as occurred in our case [23].
In summary, we describe a patient with severe gastrointestinal symptoms leading to intestinal failure from AIE, in the setting of a previous thymoma with incomplete margins, that led to the diagnosis of metastatic disease. Although autoimmune manifestations may emerge at any time through the disease continuum, relapse of symptoms requires the exclusion of tumour recurrence. TAIE is an important but rarely encountered phenomenon of thymoma, and this case reinforces the importance of a high index of suspicion, early endoscopic assessment, treatment, and nutritional support.


Comments (0)