
Remember me









This study was performed in accordance with Swedish and international guidelines for economic evaluation [20, 21]. A healthcare perspective was used, in which only healthcare-related costs were considered. No health economic analysis or statistical analysis plan was registered prior to the start of the study. In this cost–utility analysis, the addition of the NanoEcho diagnostic system to current diagnostic methods was compared with current diagnostic methods alone in terms of costs and health outcomes. The current gold standard for diagnostic methods for nodal staging of RC is MRI.
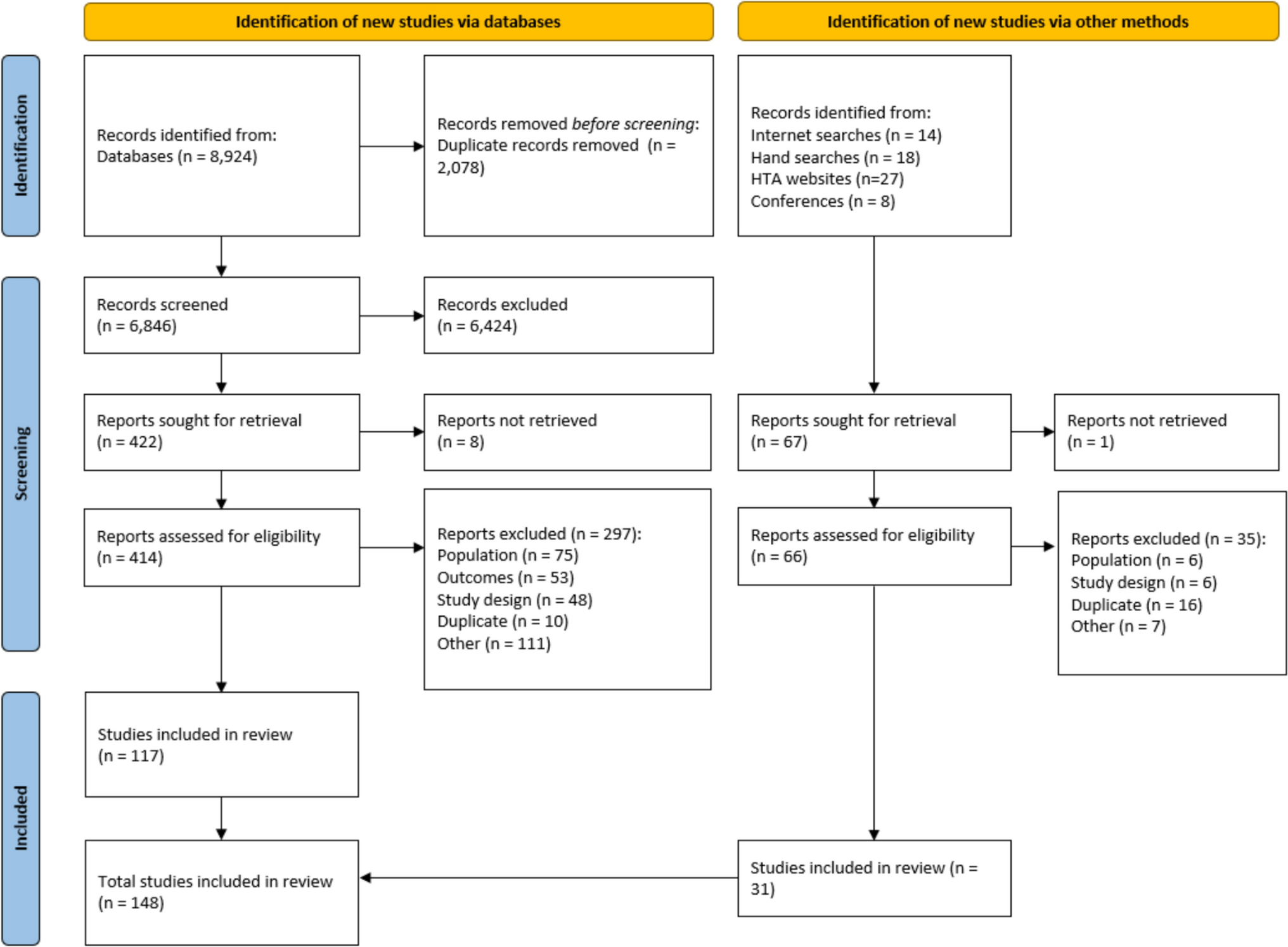
2.2 Model StructureA health economic model for diagnosis of RC was developed using Microsoft Excel. The model is not made publicly available. The model consists of a decision tree (Fig. 1A) and a Markov model (Fig. 1B). In the decision tree, the modeled cohort receive either local resection or surgical resection based on diagnostics. After the local or surgical resection, the modeled cohort enters the Markov model. This consists of a set of health states which the cohort moves between, which are determined by true lymph node status and received treatment. The probability of moving from one health state to another is determined by user-defined transition probabilities. The model uses monthly cycles and a lifetime perspective. Each health state is assigned a health-related quality-of-life weight and an associated level of resource use and costs. Further details of the treatment paths and health states included in the model are reported in following sections.
Fig. 1
Two-stage model representations: (A) Decision tree. Describes the diagnostics and treatment pathway. Patients diagnosed with false- or true-negative LNM, based on NanoEcho diagnostics, are treated with local resection. Patients diagnosed with false- or true-positive LNM, based on NanoEcho diagnostics or current clinical practise, are treated with surgical resection. (B) Long-term Markov model. Illustrates the possible transitions between health states. Patients diagnosed with false- or true-negative LNM can remain in the health state or transition to either cancer-specific death or other cause death. Patients diagnosed with false- or true-positive LNM can remain in the health state or transition to either post-operative death, cancer-specific death or other cause death. Pathological staged as LNM (pN+); Pathological staged as no LNM (pN0)
2.3 PopulationThe model analyzes two populations: the tested population, which includes all patients who will receive the NanoEcho diagnostic system in addition to current diagnostic methods, and the target population, which includes patients with clinical T1 RC and clinical suspicion of LNM who would receive surgical resection in current clinical practice and thus potentially benefit from NanoEcho diagnostic system.
Two different testing strategies were evaluated, corresponding to two alternative ways of implementing the diagnostic test in clinic. In the first strategy, the tested population was all patients newly diagnosed with RC, and in the second strategy, the tested population comprised only patients with newly diagnosed clinical T1–T2 RC.
The modeled cohort consisted of patients with and without LNM (Fig. 1A). In this model we assume that for patients with LNM, surgical resection would be the optimal treatment, and for patients without LNM, local resection would be the optimal treatment.
2.4 NanoEcho Diagnostic SystemThe value of the NanoEcho diagnostic system is the potential of correctly selecting patients in need of surgical resection (true positives) and those for whom local resection is sufficient (true negatives). Depending on the sensitivity of the NanoEcho diagnostic system, some patients would be incorrectly diagnosed with no LNM (false negatives) and receive local resection, with an increased risk of dying from RC. Depending on the specificity of the NanoEcho diagnostic system, some patients would be incorrectly diagnosed with LNM (false positives) and receive unnecessary surgical resection.
The diagnostic performance of the NanoEcho diagnostic system is still unknown and the analysis was performed at an assumed 85% sensitivity and 85% specificity that would be a reasonable and desirable performance. In addition, the sensitivity and specificity were varied between 65% and 85% to explore the added value even at a lower diagnostic performance. The value for implementing a novel diagnostic tool performing at < 65% seems not relevant.
2.5 Data SourcesInput data were based primarily on information from the Swedish Colorectal Cancer Register (SCRCR) [22]. For data not found in the register, a pragmatic literature search was performed using PubMed. When no Swedish studies were found, studies from the Nordics, Europe, and other high-income countries were used. Population characteristics for patients with RC were based on information from the SCRCR. To account for temporal variations in diagnosis rates, an annual average was calculated using data from a 5-year period (2018–2022). However, information on the number of patients in the target population was only available for 2019–2021 [23]. Assumptions and input values have been validated by two clinical experts in the field, and references are found in Table 1.
Table 1 Input values used in the health economic model2.6 Rectal CancerA population-based screening program for RC is successively being implemented in Sweden and is expected to shift the stage at diagnosis to earlier stages and thus more patients that would benefit from a better diagnostic approach to avoid surgical resection. In previous studies, T1–T2 RC increased by 6–27% after the implementation of population-based screening [23], and consequently, a 15% rise in the target population was assumed. To reflect the implementation of the screening program, the same increase was used for the number of tested patients with T1–T2 RC (in the second testing strategy). The proportion of the target population with LNM was based on a Swedish study that found that 12% of patients with early-stage clinical T1 RC who had received surgical resection had LNM on postsurgical examination of the resected tissue [6].
2.7 Surgical Complications and Postoperative MortalityRates of postoperative mortality, major complications, and permanent stoma after surgical resection of the rectum were sourced from the SCRCR [22]. Major complications were defined as those requiring more significant interventions, such as surgery or intensive care. The reported 30-day postoperative mortality rate was used in the base-case analysis, whereas 90-day postoperative mortality was tested in the sensitivity analysis. The proportion of patients with permanent stoma included patients with permanent stoma after surgical resection (57%) and patients with protective stoma that was later converted to permanent stoma (8%).
Complications following local resection in the rectum are rare and mainly managed conservatively, without the need for surgical intervention [24, 25]. Potential complications following local resection were therefore not included in the analysis, since they were assumed to have minimal impact on quality of life and health care costs.
2.8 Cancer-Specific MortalityIn addition to postoperative mortality, the model included cancer-specific mortality and other-cause mortality. Moreover, it was assumed that death from cancer was preceded by a period of metastatic disease. Age-related other-cause mortality was based on life tables from Statistics Sweden [26]. No Swedish study on cancer-specific survival that was stratified by T stage and LNM was found. Instead, an American study of 5-year survival after surgical resection, stratified by LNM, was used [27]. The 5-year survival was used to estimate a yearly cancer-specific mortality risk using a constant risk equation. The cancer-specific mortality risk was applied during the first 5 years. The risk was then set to zero to account for an expected decrease in cancer-specific mortality over time.
The modeled cancer-specific mortality for patients without LNM receiving surgical resection was based on the survival of patients with T1 RC without LNM in the American study [27]. The same cancer-specific mortality was used for local resection, as surgical resection was not expected to increase survival in patients without LNM. The cancer-specific mortality for patients with LNM receiving surgical resection was estimated from the survival of patients with T1–T2 RC and LNM stage 1–2 in the American study. The survival of patients with LNM receiving local resection is unknown, as lymph node status is based on postsurgical examination of the resected tissue. Instead, based on input from clinical experts in the field, the survival of patients with T3 RC and LNM stage 1 was used as a proxy.
2.9 Quality of LifeHealth effects were estimated as life years and quality-adjusted life years (QALYs). The disutility for surgical resection was based on a multinational study reporting quality of life measured by EQ-5D in patients with RC before and 4 weeks after open surgical resection [28], and it was assumed that the disutility would last for 2 months after surgical resection. Information of the disutility due to permanent stoma was obtained from a recent Spanish study reporting EQ-5D 1 year after surgical resection [29]. The duration of the disutility due to permanent stoma was based on a Swedish study that reported disutilities due to permanent stoma up to 7 years after surgical resection [30]. The total QALY loss associated with metastatic disease was sourced from a health economic evaluation of population-based screening for colorectal cancer by the Swedish National Board of Health and Welfare [31].
2.10 Healthcare CostsAll costs were calculated in Swedish kronor (SEK) at the 2023 price level. Costs for the NanoEcho diagnostic system healthcare visits, major complications, and permanent stoma were sourced from the price list of the Southern healthcare region in Sweden [32]. Costs for the NanoEcho diagnostic system healthcare visits were assumed to correspond to two physician visits in the gastroenterology department.
Healthcare costs for local resection and surgical resection were based on information from the cost-per-patient database (KPP) held by the Swedish Association of Local Authorities and Regions [33]. The average cost for local resection and surgical resection were calculated using procedure codes and mean cost per healthcare episode (procedure codes are presented in Supplementary Table 1, see electronic supplementary material [ESM]).
Major complications typically require inpatient care, and healthcare costs were assumed to be equivalent to the cost of 4 days of inpatient care in the gastroenterology department, based on the average number of days spent in inpatient care in 2021.
Costs for healthcare visits related to permanent stoma were applied during the first year with permanent stoma, and the number of visits was based on a Swedish report of national guidelines for healthcare related to stoma [34]. The cost per healthcare visit was assumed to be equivalent to the cost of one nurse visit in outpatient care in the gastroenterology department [32]. The annual cost of stoma equipment was applied each year with permanent stoma and sourced from a report by the Dental and Pharmaceutical Benefits Agency in Sweden, adjusted to 2023 price levels [31, 35].
Costs for metastatic disease were sourced from the evaluation of population-based screening for colorectal cancer by the National Board of Health and Welfare and adjusted to 2023 prices [36]. A yearly discount rate of 3% was used to discount all simulated costs and health benefits according to Swedish recommendations [21].
2.11 OutcomesModel outputs were calculated for the addition of the NanoEcho diagnostic system to current rectal diagnostic methods, current diagnostic methods alone, and the increment between them. Model outputs included the number of tested patients per patient in the target population, given treatments, complications and deaths from surgical resection, RC or other causes. Costs and QALYs were calculated based on modeled events.
The price of the NanoEcho diagnostic system is not yet known. Therefore, the potential value, or economically justifiable price [37], of the NanoEcho diagnostic system was estimated. The justifiable price was first calculated at a cost-neutral level, resulting in no increase in healthcare costs. It was then calculated at a willingness to pay (WTP) of 500,000 SEK/QALY, representing the threshold between moderate and high cost per QALY according to the Swedish National Board of Health and Welfare [38]. The robustness of the results was tested using one-way sensitivity analyses.
Comments (0)