A case of IgG-type heavy chain amyloidosis with membranous nephropathy-like changes with long-term survival
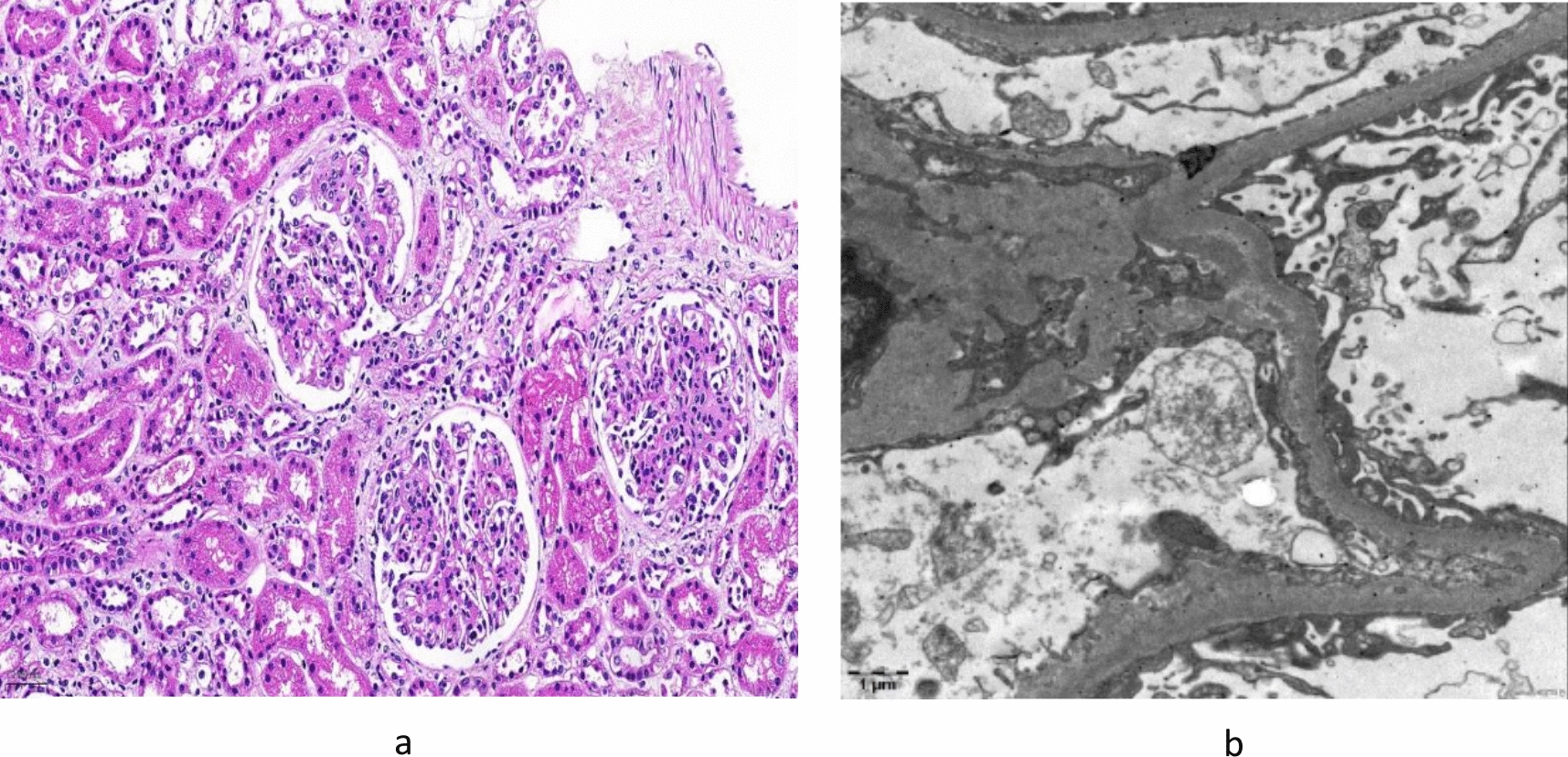
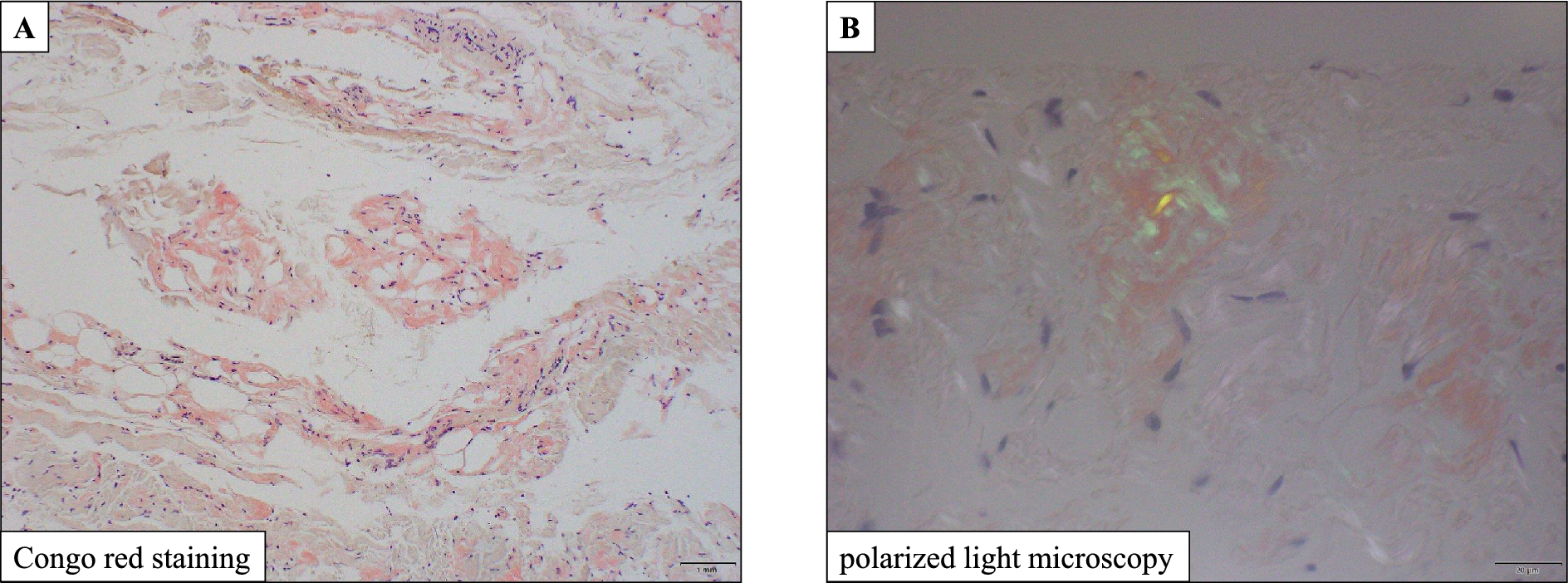
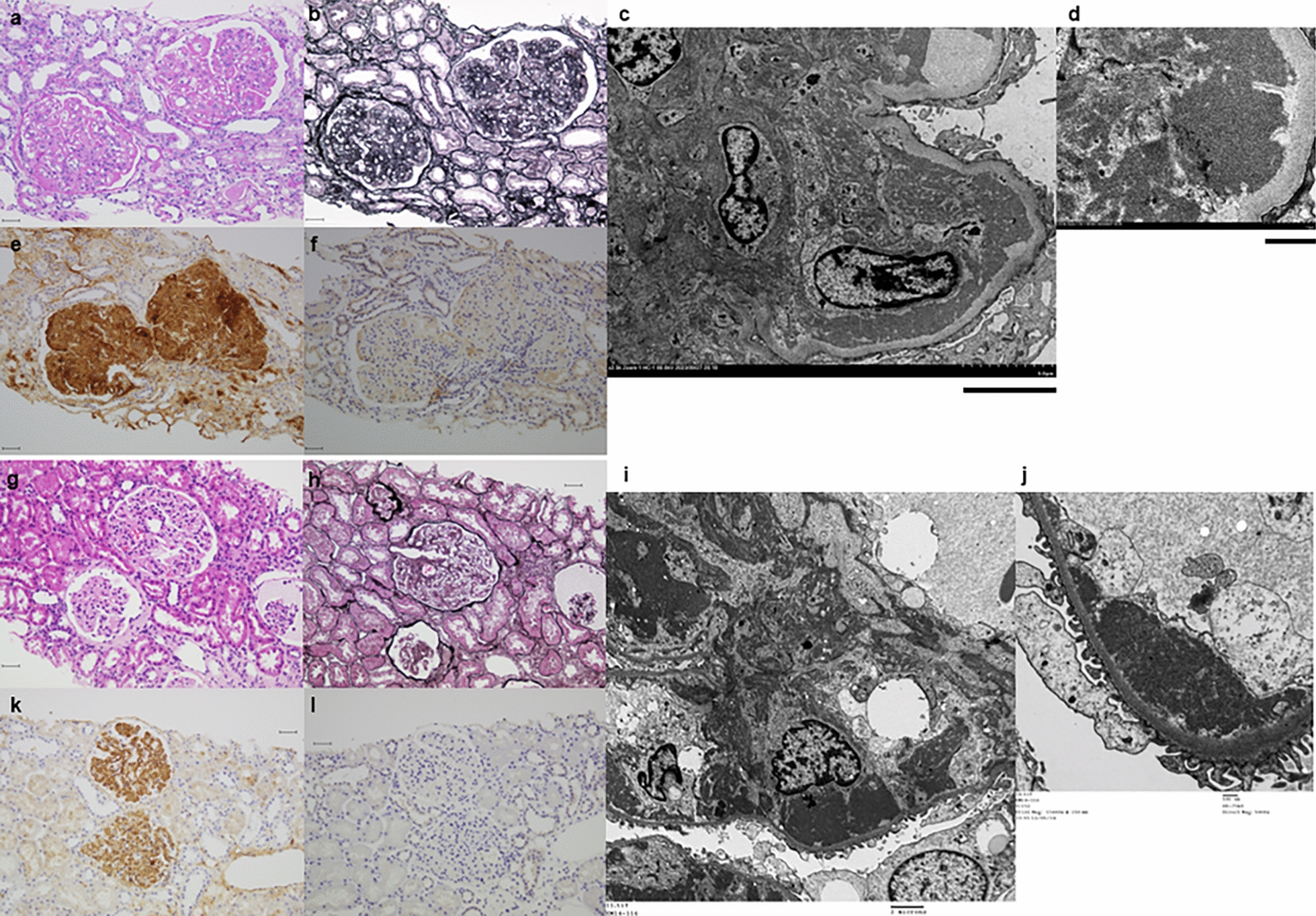
We performed a kidney biopsy on a 68-year-old man with 2.6 g/day proteinuria. Immunofluorescence (IF) study showed a positive finding of IgG (IgG1) along the glomerular capillary wall, suggesting membranous nephropathy. However, electron microscopy showed no subepithelial electron dense deposits and amorphous deposits of 8–12 nm fibrillar structure, and positive DFS/Congo red staining confirmed the diagnosis of amyloidosis. Amyloid deposits were localized only in the glomeruli. No overt extrarenal amyloid lesions were identified. Serum and urine were positive for monoclonal IgG-lambda, but IF was negative for kappa and lambda, ruling out AL-amyloidosis. At 75 years of age, he underwent a second kidney biopsy, and the IgG-positive findings at IF became more pronounced, with progressive glomerular sclerosing lesions. A proteomic analysis was performed focusing on the positive IgG finding in IF. The amyloid was proven to be composed of fragments of a heavy chain variable region sequence. AH-amyloidosis was the final diagnosis. He was treated according to the treatment for AL-amyloidosis, but hemodialysis was started at the age of 81, and died at the age of 86. We report a valuable case of AH-amyloidosis with an observed long-term prognosis.






Comments (0)