
Remember me





The patient is an eight-year-and-four-month-old female child who was admitted to the hospital on May 31, 2021, presenting with a four-day history of rash on both lower limbs and a two-day history of abdominal pain. Four days prior to admission, the patient developed a rash primarily concentrated on the calves of both lower limbs, characterized by erythematous papules elevated above the skin surface. In some areas, the rash coalesced into patches, without accompanying symptoms, such as itchiness, abdominal pain, joint swelling, or hematuria. Two days before admission, the patient experienced abdominal pain, which gradually intensified and was primarily localized around the umbilical region. There were no associated symptoms of vomiting, diarrhea, hematochezia, edema, or oliguria. The patient’s past medical history, personal history, and family history did not reveal any significant findings.
Physical examination results indicated that the heart sounds were normal, exhibiting a regular rhythm and an absence of any pathological murmurs. Breath sounds were clear in both lungs, without the presence of dry or wet rales. The abdominal region was soft, accompanied by mild tenderness in the vicinity of the umbilicus. No rebound tenderness was noted, and neither liver nor spleen was palpable. The neurological examination revealed no abnormalities. Additionally, no edema was observed throughout the body. However, dark red circular papules were visible on both lower limbs, which did not diminish upon the application of pressure.
On June 1, 2021, a routine urine test revealed microscopic hematuria accompanied by mild proteinuria, leading to the diagnosis of IgAVN. More laboratory test results are detailed in Table 1. Anti-nuclear antibody and anti-neutrophil cytoplasmic antibody were both negative. Ultrasound of the urinary system revealed no abnormalities. Gastroscopy indicated scattered ecchymoses and patchy erosions on the mucosa of the gastric antrum, duodenal bulb, and descending duodenum. During the period of hospitalization, the child exhibited significant hematuria and an elevation in the quantification of urinary protein to 2544.7 mg per 24 h. At the onset of the disease, the patient’s serum albumin level was 44.6 g/L. However, as the disease progressed, the serum albumin levels continued to decline, reaching a minimum of 26.9 g/L.
Table 1 Demographic and clinical baseline characteristics of patientsThe pathological analysis conducted following a renal biopsy on August 10, 2021 revealed mesangial cell proliferation and an increased mesangial matrix within the glomeruli with no observed thickening of the capillary basement membrane. Out of the 26 small glomeruli examined, approximately 7 exhibited mild adherence to the Bowman’s capsule, and one glomerulus examined cellular crescent bodies. There was mild granular degeneration of tubular cells, with no tubular atrophy, interstitial edema, fibrosis, scattered lymphatic mononuclear smooth muscle cells, and no interstitial blood vessels. In the frozen sections, nine small glomeruli were noted, with lgG -, lgA + + + , lgM + , C3 + , C4-, C1q -, and positive branching deposits of Fib + in the mesangial area. Type IV collagen detection revealed no abnormalities in the distribution of a2 and a5 chains. Electron microscopy indicated no significant thickening of the glomerular basement membrane, with most foot processes being fused, and electron-dense deposits were observed in the mesangial area, findings consistent with IgAVN type IIIb, as depicted in Fig. 1.
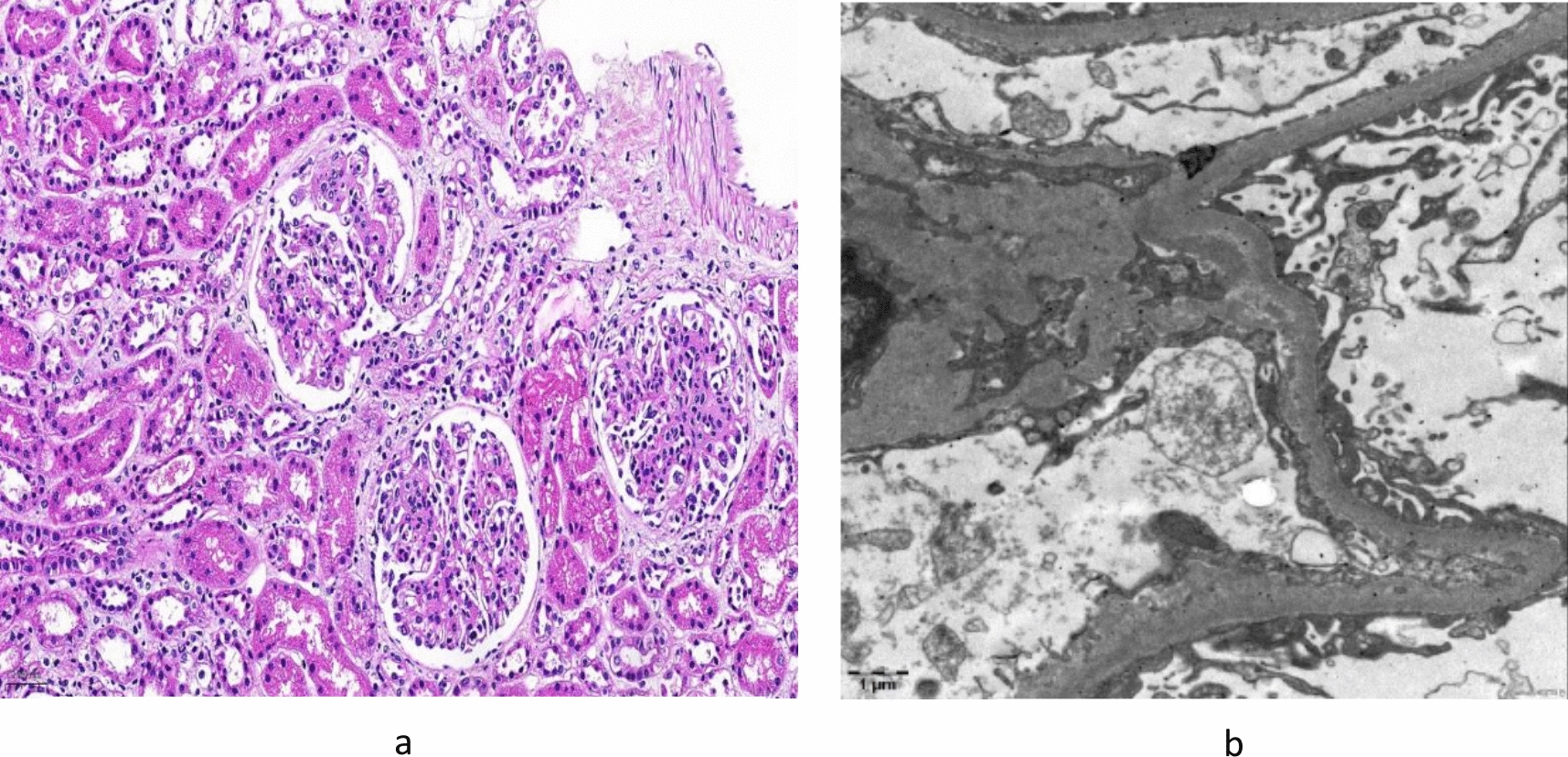
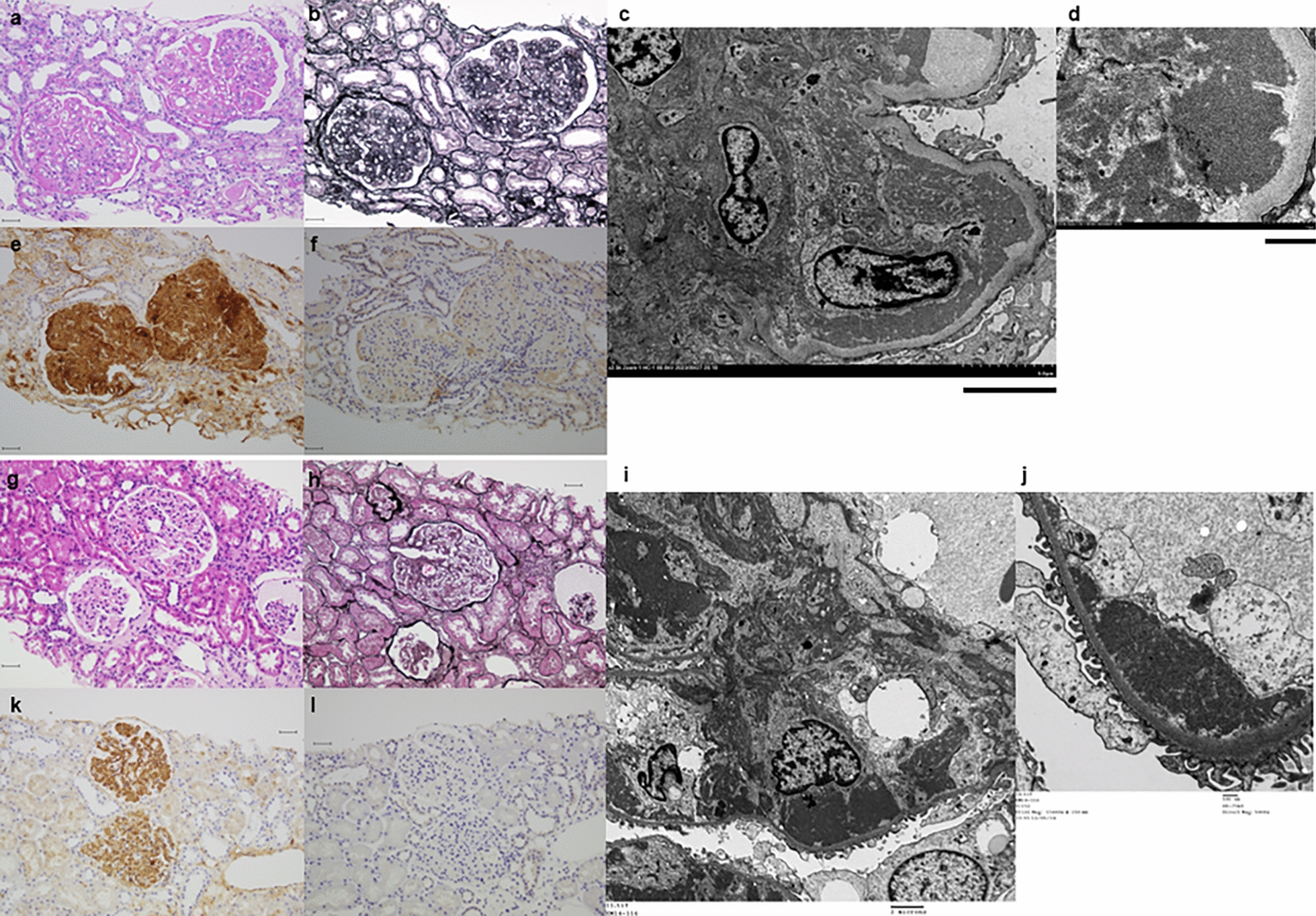
Fig. 1
Pathological manifestations of kidney tissue under light microscopy (August 2021). a Mesangial cell proliferation, mild adhesion between the glomerulus and Bowman's capsule, with cellular crescents visible (HE, × 200). b Most foot processes fused, with electron-dense deposits seen in the mesangial area (EM)
Subsequently, she underwent treatment with MP pulse therapy and intravenous CTX. Upon the completion of eight cycles of CTX treatment, amounting to a total dosage of 3.2 g, the child continued to display significant hematuria. Routine urine analysis revealed an elevated red blood cell count of 1005.4 /uL and a urine protein quantification of 1119.06 mg/24 h. Commencing in December 2021, CTX was stopped and MMF was administered orally in two doses, totaling 0.75 g/d, with the blood drug concentration kept within normal limits. MMF was orally administered for a duration of four months, during which the 24-h urine protein consistently surpassed 1000 mg. Considering the poor effect of MMF, the child went to another hospital for treatment and was treated with 10 mg/d of leflunomide (LEF) in May 2022. After two months of oral LEF administration, an improvement in hematuria was noted compared to the previous condition, with the urine red blood cell count decreasing to 300/μL. However, the urine protein quantification remained at 1014 mg/24 h. Despite undergoing a series of treatments with glucocorticoids and three immunosuppressive agents over a one-year period, the patient’s urinary protein quantification remained elevated, exceeding 1000 mg/24 h. Given the ineffectiveness of various prior drug therapies, it was noted that the peripheral blood CD19 + B cell counts were 393/μL. On July 18 and 25, 2022, RTX was administered twice at a dosage of 375 mg/m2, respectively. Subsequent to the RTX treatment, the child’s gross hematuria resolved, with the urinary protein quantification decreasing to 731.3 mg/24 h, and the peripheral blood CD19 + B cell counts decreasing to zero. Between August and October 2022, she continued to experience intermittent episodes of gross hematuria and repeated urinalysis indicated a urine protein level of 2 + ~ 3 + . The child experienced two urinary tract infections accompanied by significant gross hematuria, during which time the serum immunoglobulin IgG level was measured to be 3.0 g/L, with the peak urine red blood cell count reaching 773/μL. After the administration of antibiotics, the symptoms of gross hematuria were alleviated. Subsequently, the patient received 20 g of immunoglobulin for immune support therapy, resulting in a significant reduction in the urine red blood cell counts to 64.9/μL. However, there was a recurrence in urinary protein quantification, which increased to 1823.1 mg/24 h. The child was then treated at the Children’s Hospital affiliated with Fudan University and restarted oral MMF at a dosage of 0.75 g/d combined with traditional Chinese medicine in December 2022. The amount of urinary protein continued to rise. Due to the consistent increase in the amount of urine protein, RTX was administered again on March 7th and 15th, 2023. However, RTX didn’t work very well. In July 2023, dapagliflozin was added at a dosage of 5 mg/d, in conjunction with oral MMF and fosinopril. During the entire medication period, renal function remained normal, but continuous microscopic hematuria accompanied by moderate to severe proteinuria was observed. The detailed medication process and the follow-up data are presented in Fig. 2.
Fig. 2
The relationship between follow-up data and treatments. MP: Pulses of intravenous methylprednisolone; CTX: Cyclophosphamide; MMF: Mycophenolate Mofetil; RTX: Rituximab; LEF: Leflunomide; eGFR: Estimated glomerular filtration rate
In October 2023, subsequent to an infection of the upper respiratory tract, the patient exhibited symptoms of hematuria, with a urine red blood cell counts elevating to 967.6/μL and a urinary protein quantification of 2582 mg/24 h. After a thorough evaluation to exclude any contraindications, treatment with telitacicept was initiated on October 21, 2023, at a dosage of 80 mg per injection, administered subcutaneously once weekly. After one month of telitacicept administration, the patient’s urinary protein quantification decreased to 837.9 mg/24 h, and the urine red blood cell counts decreased to 124.3/μL. By 12 weeks of telitacicept treatment, the patient’s routine urine test indicated that protein was negative. In January 2024, the patient was able to successfully reduce steroid dosage, and in April 2024, MMF was discontinued. After 10 months of telitacicept treatment, no significant gross hematuria was observed in the patient, and the urine red blood cell counts had decreased substantially to 27/μL. Furthermore, urine protein levels were effectively controlled and maintained within a range of 127 mg/24 h to 207 mg/24 h (Fig. 2). Specifically, the levels of immunoglobulin (IgA, IgM, IgG) did not show a significant decrease during the treatment with telitacicept (Fig. 3).
Fig. 3
Follow-up of immunoglobulin levels
Upon initiating telitacicept therapy, the initial count of peripheral blood CD19 + B cells was documented as 1.63/μL. Following the administration of telitacicept, the monitored count of peripheral blood CD19 + B cells gradually increased, ultimately reaching a final count of 51.43/μL. Throughout the entire duration of treatment and subsequent follow-up, no life-threatening serious adverse events, including severe infections or anaphylactic shock, were noted. Throughout the course of the illness, the levels of blood creatinine, cystatin C, urine α1-microglobulin, and urine β2-microglobulin remained within normal range. Furthermore, the patient’s blood pressure and the renal function were also determined to be within normal ranges. As illustrated in Fig. 2, the patient’s eGFR decreased at week 25 following treatment with telitacicept, which was attributed to the viral gastroenteritis the patient experienced at that time. Given the presence of prerenal acute kidney injury during that period, the patient’s eGFR improved after the administration of fluid therapy. During the period of telitacicept therapy, the patient did not experience any weight gain, but did exhibit a growth in height by 2 cm.
Comments (0)