
Remember me




Ethical approval was obtained from the local ethical committee (BASEC-Nr. 2023-00703) for this retrospective study. Consent was obtained for evaluation of existing imaging data and the HIPAA privacy rules were applied. Eighty consecutive patients who underwent thoraco-abdominal MRI on a 1.5-T scanner (Signa Artist, GE HealthCare, Waukesha, WI) at our institution employing PROPELLER sequences with DL-based image reconstruction were considered for this study. The inclusion criterion was the availability of a previous thoraco-abdominal MRI examination with conventionally reconstructed PROPELLER sequences to enable comparison of scan time between the previous PROPELLER protocol and the current accelerated PROPELLER protocol.
Imaging protocol and post-processingThe patients underwent thoraco-abdominal imaging with multichannel surface coils (AIR™ Coil, GE HealthCare, Waukesha, WI) covering the chest and abdomen. The routine protocol included a 3-dimensional (D) short tau inversion recovery fast spin echo sequence (CUBE) and diffusion-weighted imaging, axial and coronal T1-weighted PROPELLER sequences, and respiratory-gated axial T2-weighted PROPELLER with fat saturation. After intravenous injection of a single dose of gadolinium-based contrast agent (gadoteric acid, Dotarem, Guerbet AG, Zürich, Switzerland), a dynamic 3-D acquisition (DISCO) was followed by a 3-D T1-weighted fast gradient echo sequence (LAVA).
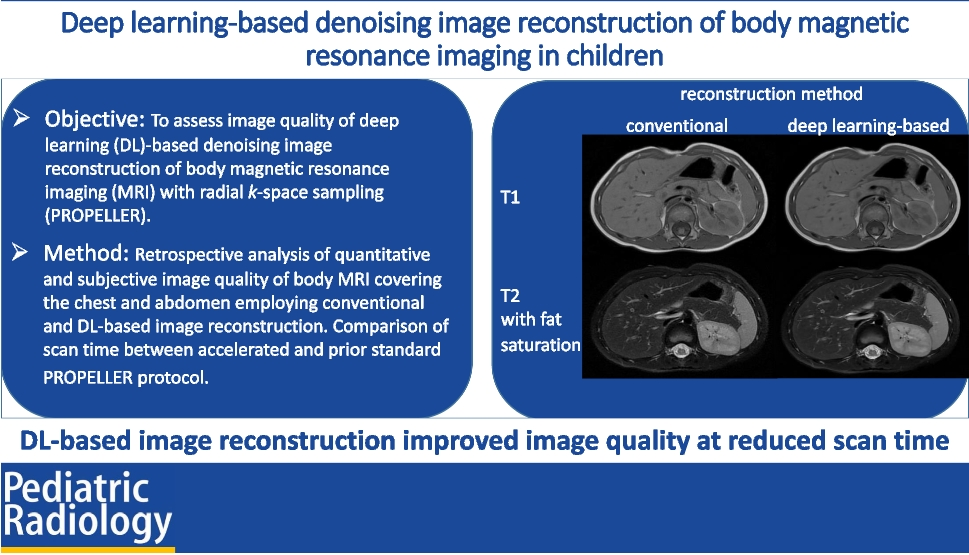
Subjects of this study were the T1-weighted and T2-weighted axial PROPELLER images obtained before contrast administration. The PROPELLER sequences in this study were acquired with higher image matrix and less signal averages than in our previous standard protocol (scan parameters are given in Table 1). Scan time was extracted from MRI scanner internal timing, which is saved to digital imaging and communications in medicine (DICOM) meta data, and is reported here as seconds per slice for normalisation. By the time of the study, the DL-based image reconstruction algorithm (AIR™ Recon DL, GE HealthCare, Waukesha, WI) was provided by the vendor as a research option for paediatric body imaging. The reconstruction pipeline includes a residual neural network that was trained to reduce the noise and truncation artefacts and improve edge sharpness from the raw blade-combined images. The convolutional residual network was trained with a supervised learning approach using pairs of near-perfect, high-resolution, and conventional images [15, 19, 20]. The model was integrated into the conventional PROPELLER reconstruction pipeline, generating conventional and DL-reconstruction images from the same acquisition. The impact of DL-reconstruction on the image quality in comparison to the conventional approach was evaluated. Scan times from the current PROPELLER acquisitions were compared to those from a prior examination acquired with our old standard PROPELLER protocol.
Table 1 Technical settings of standard and accelerated PROPELLER sequences for paediatric body magnetic resonance imagingQuantitative image assessmentSignal-to-noise ratio (SNR) of the liver and spleen and contrast-to-noise ratio (CNR) of the liver and spleen in comparison to spinal musculature were calculated to assess quantitative image quality.
SNR is calculated as the ratio of signal intensity (SI) of the organ parenchyma to the standard deviation (SD) of the signal intensity of the background – SD air. CNR is defined as the difference in signal contribution (SI) of the tissue of interest and a reference tissue, divided by SD air.
$$\mathrm=\frac\;\left(\mathrm/\mathrm\right)}\left(\mathrm\right)}\quad \mathrm=\frac\;\left(\mathrm/\mathrm\right)-\mathrm\;\left(\mathrm\right)}\;\left(\mathrm\right)}$$
Measurements were made within circular regions of interest (ROI) of diameters ranging from 9.1 mm to 10.6 mm (area ranging from 65 mm2 to 89 mm2) within the liver and spleen parenchyma omitting the vasculature and within the air next to the body. If technically possible, the ROIs in the liver, spleen, and air were positioned in the same line on the x-axis. To determine the CNR, autochthonous spinal muscles were chosen as tissue of reference. The ROI was positioned at the identical location of the organ, muscle, and air on the T1-weighted and T2-weighted images. The example of ROI placement is given in Fig. 1.
Fig. 1
Example of region of interest placement on an axial deep learning-reconstructed T2-weighted PROPELLER image before contrast agent administration to determine signal-to-noise ratio and contrast-to-noise ratio
Qualitative image assessmentPrior to the data analysis, the images with conventional and DL-reconstruction were anonymised, and the sequence information was removed. The images were independently reviewed by three board-certified paediatric radiologists (C.J.K. with 30 years, V.P. with 13 years, and M.Z. with 8 years of experience) in random order, and the observers were blinded to the patient clinical data. The images were evaluated for the presence of noise, motion artefact, visibility of the peripheral lung vessels and subsegmental bronchi at the lung bases, abdominal organ margins, and visibility of the peripheral liver and spleen vessels using a 4-point Likert scale.
The degree of noise was scored with 3=no noise, 2=mild noise, 1=noise potentially obscuring the vessels, and 0=not diagnostic. The motion artefact was evaluated as follows: 3=no artefact, 2=mild, 1=moderate, 0=severe. The observers assessed the visibility of peripheral lung vessels (1 cm subpleural), subsegmental bronchi and peripheral liver, and spleen vessels in a following manner: 3=well seen with sharp margins, 2=well seen, blurred, 1=hardly visualised, 0=not visualised. Margins of the abdominal organs were scored with 3=well seen with sharp margins, 2=well seen, blurred, 1=hardly visualised, and 0=not visualised.
For each sequence and corresponding reconstruction method, six image quality items were evaluated by three observers and used for the cumulative image quality score. The median of the cumulative image quality score from three readers was used for comparison between reconstruction types.
StatisticsThe primary analysis showed that the data does not follow a normal distribution. All data collected for the quantitative and the qualitative image assessment were compared using the Wilcoxon signed-rank test. A statistical significance of P-value <0.05 among the reconstruction methods for each sequence has been determined. The reliability of agreement for image quality between the three readers was determined by interclass correlation coefficient (ICC). ICC values of <0.5 indicated poor, between 0.5 and <0.75 moderate, between 0.75 and <0.9 good, and between 0.9 and 1 excellent agreement. Statistical analysis was conducted using the software XLSTAT, version 2023.1.1 (Lumivero (2025); XLSTAT statistical and data analysis solution, New York, NY; https://www.xlstat.com/en) and MedCalc® Statistical Software version 23.1.6 (MedCalc Software Ltd, Ostend, Belgium; https://www.medcalc.org; 2025).
Comments (0)