Olfactory, subfrontal, or olfactory groove schwannoma is a very rare entity, with only six pediatric cases reported worldwide, whose origin is not yet fully understood [1, 5]. Two main theories have been proposed to explain its development. The developmental theory suggests that mesenchymal pial cells transform into ectodermal Schwann cells or that neural crest cells might migrate to these regions. The non-developmental hypotheses defend that these schwannomas arise from Schwann cells present in adjacent structures, such as the anterior ethmoidal nerve, nerve plexus, or meningeal branches of the trigeminal nerve. Another possibility is that Schwann cells could arise from multipotent mesenchymal cells following injury [2, 5].
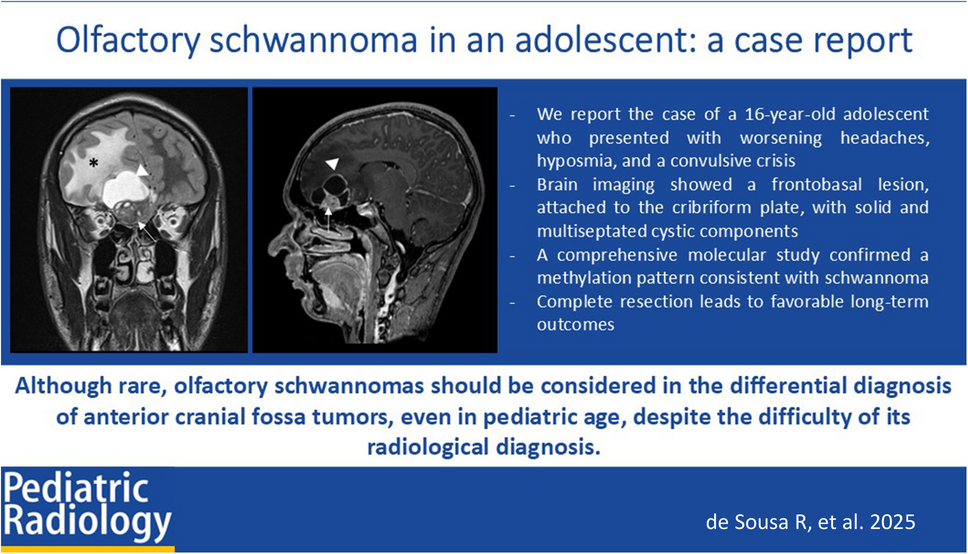
The most common manifestations of olfactory schwannomas include headache, anosmia, and seizures, all of which were present in our patient [1, 2, 5]. As they are located in the anterior fossa in relation with the olfactory system, olfactory dysfunction is a common clinical manifestation. Nevertheless, there are reported cases of preserved olfactory function [3]. Headache and seizures result from increased intracranial pressure.
The average age of onset for olfactory schwannomas is 33 years old, which contrasts with the age of our patient. These tumors are more frequent in males [1].
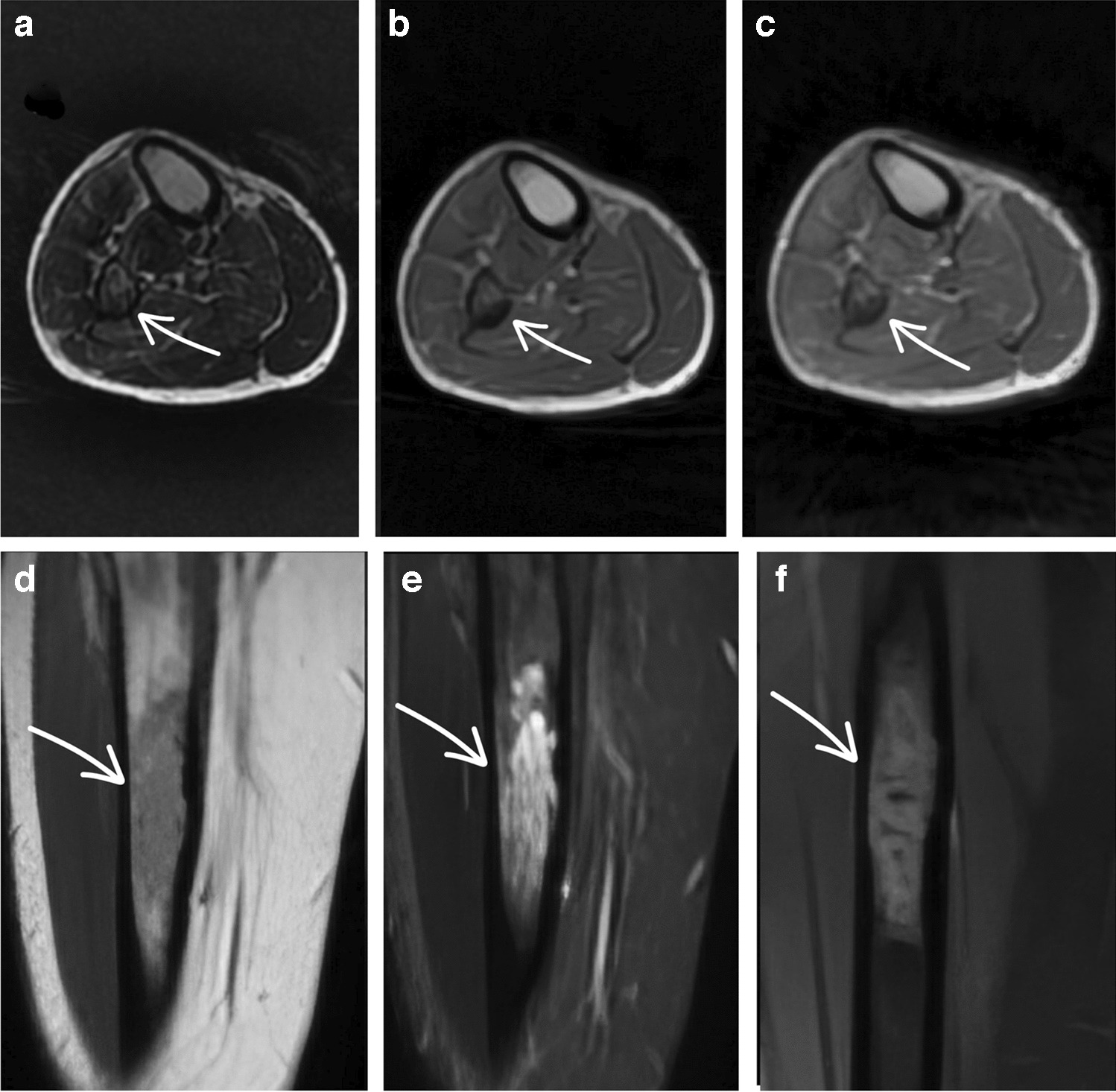
Schwannomas present as an iso- or hypodense mass on CT. On MRI, they can be iso- or hypointense on T1WI and heterogeneously hyperintense on T2WI, often with prominent heterogeneous contrast enhancement, particularly in larger tumors due to cystic areas [4, 6].
Preoperatively, olfactory schwannomas are frequently misdiagnosed as olfactory groove meningiomas, olfactory neuroblastomas, or dural-based metastases, the most frequent differential diagnosis for extra-axial anterior fossa neoplasms [1, 2, 6].
Some bone erosion or remodeling, and multiple low signal foci on T2*, related to microbleeds, seem to be more indicative of schwannomas rather than meningiomas, which typically show bone sclerosis and a dural tail [4, 6]. These differentiating features were not present in our case. Aggressive bone destruction and invasion of adjacent structures are warning features suggesting sinonasal malignant neoplasms.
The distinction between olfactory schwannomas and olfactory ensheathing cell tumors remains challenging, as they appear in the same topography and exhibit the same radiological features. Further molecular markers are needed for better discrimination. The latter is even rarer, as the olfactory ensheathing cells, the glial cells that cover the axons of the olfactory nerve, appear to be resistant to neoplastic transformation [6, 7].
Given the benign nature of olfactory schwannomas, the treatment of choice is complete surgical resection of the tumor, with no need for adjunctive therapy. After complete resection, the prognosis tends to be favorable [3, 7].
Although rare, olfactory schwannomas should be considered in the differential diagnosis of anterior cranial fossa tumors, even in pediatric age, despite the difficulty of its radiological diagnosis.





Comments (0)