This study aimed to investigate longitudinal changes in renal function and CMT during anti-VEGF therapy for DME. Our findings contribute to current knowledge by providing insights into the relationship between renal function, DME, and treatment outcomes. First, we observed a mean total of 5.3 anti-VEGF injections per eye over the course of 3 years (first year: 3.0, second year: 1.6, third year: 0.7). Compared with other real-world studies, such as STREAT-DME in Japan [13] (4.3 injections over 2 years), LUMINOUS (conducted in over 43 countries, including regions in Asia, Europe, North America, Latin America, and Oceania) [14] (4.5 injections over 1 year), MERCURY in Japan [15] (4.9 injections over 2 years), and Talks SJ et al. in the UK [16] (12 injections over 3 years), our study demonstrates an injection frequency comparable to those observed in the studies conducted in Japan. This consistency in the treatment frequency reflects the standard practice of managing DME using anti-VEGF therapy in a real-world setting in Japan.
Regarding visual outcomes, our study shows a mean improvement of − 0.07 logMAR over 3 years. This improvement is consistent with the findings from STREAT-DME (change of − 0.09 logMAR/2 years), LUMINOUS (change of − 0.07 logMAR/1 year), and MERCURY (change of − 0.13 logMAR/2 year). Notably, each study had a different follow-up duration [14, 15]. Nonetheless, these findings collectively highlight the efficacy of anti-VEGF therapy in improving the visual acuity in patients with DME. Comparing our results with those of previous studies, we observed similar treatment responses in terms of injection frequency and visual outcomes.
In our study, we found that 72.6% of the patients at baseline and 83.9% at 36 months after anti-VEGF therapy had stage 2 or higher CKD. This is comparable to Busch et al., who report that 83% of patients with DME had stage 2 or higher CKD [17]. The high prevalence of CKD in patients with DME highlights the close association between renal function impairment and the development or worsening of DME. These findings emphasize the importance of monitoring renal function in patients with DME and underscore its potential role in predicting DME exacerbation. The mechanism by which CKD exacerbates DME includes decreased plasma colloid osmotic pressure due to urinary protein excretion, elevated circulating levels of VEGF and inflammatory cytokines, disruption of the blood-retinal barrier, and increased vascular permeability [18,19,20,21,22]. Together, these factors contribute to the progression and worsening of DME in patients with impaired renal function.
Although we only analyzed serum Cre, eGFR as markers of renal function, additional indicators—such as urinary protein and the urinary albumin-to-creatinine ratio (ACR)—are also associated with the risk of developing diabetic macular edema (DME) [3,4,5, 23, 24]. Further studies are warranted to identify which specific indicators have the most significant impact on the pathogenesis of DME and DR.
Renal function impairment and responsiveness to anti-VEGF therapy in DME
Our study findings reveal that, although there was no significant association between baseline renal function (serum Cre levels and eGFR) and both visual and morphological outcomes in patients with DME undergoing anti-VEGF treatment, the presence of stage 3 or higher CKD at 36 months was significantly associated with greater fluctuations in CMT.
Although there are several reports on the association between renal function and responsiveness to anti-VEGF therapy for DME, the findings vary, and a consistent consensus has not yet been established, as detailed below. (1) Reports indicating no significant impact of baseline renal function on DME treatment outcomes: A randomized controlled trial of monthly ranibizumab (RISE/RIDE) found that serum Cre and eGFR levels did not affect visual prognosis [12]. (2) Reports indicating a negative impact of decreased renal function on DME treatment outcomes: In a PRN study of conbercept, baseline urinary ACR was positively correlated with CMT and injection frequency [10]. Following three ranibizumab injections, cases with lower eGFR showed a higher presence of subretinal fluid [9]. Post-bevacizumab, reductions in CMT were significantly smaller in cases with higher BUN and Cre values and lower eGFR [25], High baseline urinary ACR cases showed significantly greater CMT fluctuations with PRN therapy (DRCR Protocols T, V) [26]. (3) Reports indicating that decreased renal function positively impacted DME treatment outcomes: In a PRN study with ranibizumab, patients with macroalbuminuria (urinary ACR > 300mg/g) showed significantly greater CMT improvements compared to those with urinary ACR < 30 mg/g [11]. In our study, baseline CKD stage (whether stage 3 or higher or lower) did not significantly affect visual outcomes, maximum CMT during follow-up, or CMT fluctuation at 36 months. However, at 36 months, patients with stage 3 or higher CKD showed significantly greater maximum CMT and fluctuations compared to those with CKD below stage 3.
The finding that baseline renal function did not affect visual prognosis aligns with Singh et al. [12] and our observation of comparable CMT improvements in cases with poor baseline renal function echoes Lai et al. [11]. However, our results differ from Liu et al. [10], Tsai et al. [9], Hwang et al. [25], and Torjani et al. [26], who report that poorer baseline renal function was associated with lesser CMT reduction, greater fluctuation, and increased injection frequency with anti-VEGF treatment. Notably, Torjani A et al. and Liu ZY et al. used baseline urinary ACR as an indicator. While urinary ACR was not analyzed in our study, it is an early marker of diabetic nephropathy, indicating early DKD. Our study likely included cases with early DKD at baseline that progressed to stage 3 CKD with decreased eGFR during follow-up. Thus, future investigations incorporating early nephropathy markers like baseline urinary ACR are warranted to track long-term renal function changes.
Improvement of DME with dialysis
Dialysis initiation for end-stage renal failure is reported to improve DME [27, 28]. The mechanisms underlying the improvement in DME after dialysis initiation include resolution of choroidal edema, improvement of plasma colloid osmotic pressure, resolution of uremic conditions such as hypertension and anemia, and reduction in circulating inflammatory cytokines and growth factors. As previously reported, in our study, all patients who required dialysis during the follow-up period showed a significant decrease in CMT after dialysis initiation, with only one patient requiring additional anti-VEGF injections.
Renal function deterioration during Anti-VEGF treatment
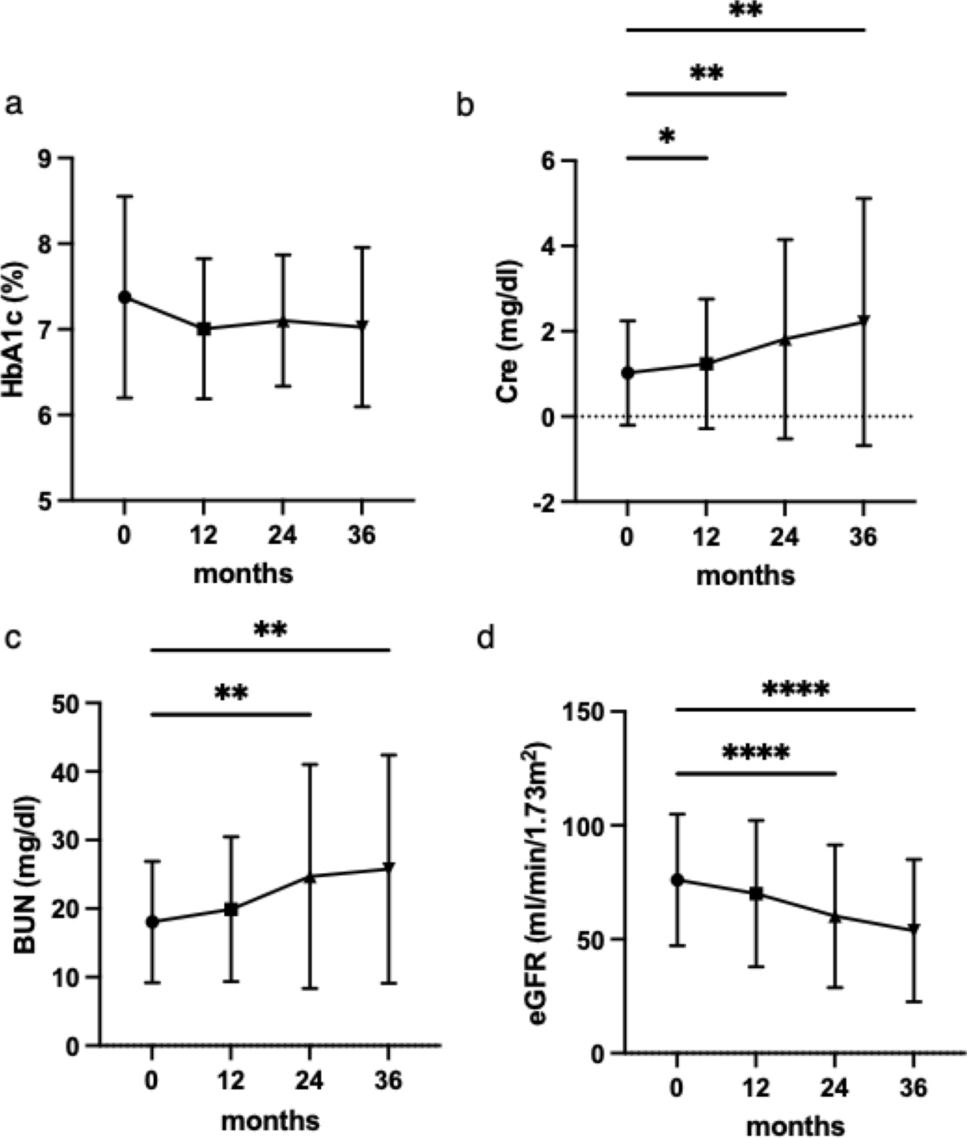
The annual progression rates from DKD stages 1 to 2, stages 2 to 3, and stages 3 to 4 are reported to be 2%, 2.8%, and 2.3%, respectively, low compared to those in our study [29]. The accelerated progression rate of DKD in this study compared to the general diabetic population can be attributed to two factors: (1) this study focused on patients with DME and DR, both known risk factors for renal function deterioration. Park et al. report that the risk of CKD progression was 2.9 times higher in patients with non-proliferative retinopathy at baseline and 16.6 times higher in patients with proliferative retinopathy at baseline [8]. Additionally, Moriya et al. report that patients with microalbuminuria and retinopathy showed a greater decline in eGFR, suggesting that CKD with DME may progress more rapidly [7].
(2) Considering previous reports on the impact of anti-VEGF agents on renal impairment, it is possible that intravitreal anti-VEGF therapy may have contributed to the worsening of renal function over the course of follow-up. Several reported cases show that some individuals experience decreased eGFR and developed proteinuria after receiving anti-VEGF intravitreal injections, and subsequent renal biopsies revealed glomerular pathological abnormalities such as focal segmental glomerulosclerosis, minimal change disease, and thrombotic microangiopathy [30, 31]. VEGF secreted by podocytes in the glomerulus plays a crucial role in maintaining endothelial cell function. Systemic VEGF inhibition can disrupt podocyte function, leading to a decline in glomerular function [32]. In this study, eight cases progressed to dialysis during follow-up, exhibiting a rapid decline in renal function (Table 5), suggesting that the impact of anti-VEGF therapy on accelerating renal function decline cannot be ruled out. Although there are some case reports on the systemic effects of intravitreal anti-VEGF injections, it remains uncertain whether these effects are directly attributable to the injections.
Limitations
The retrospective nature of our study introduces potential biases and limitations in the data collection and analysis. Additionally, the relatively small sample size and single-center design may limit the generalizability of our findings. The observational design of this study prevents us from establishing causality between renal function impairment and DME development or worsening. Moreover, the lack of long-term follow-up data limits our understanding of the sustained effects of anti-VEGF therapy and dialysis on DME and renal function. Furthermore, this study was conducted in a real-world setting, where the likelihood of undertreatment was potentially present.
This retrospective observational study provides valuable insights into longitudinal changes in renal function and CMT during anti-VEGF therapy for DME. Our findings highlight the high prevalence of renal function impairment in patients with DME and a marked progression of renal impairment was observed during the course of anti-VEGF therapy. Renal function parameters may influence DME fluctuation. Furthermore, dialysis initiation in patients with end-stage renal failure can lead to an improvement in DME. These findings emphasize the importance of monitoring renal function. Caution should be exercised regarding potential renal complications associated with anti-VEGF intravitreal injections. Further research is required to elucidate the complex relationship between renal function, DME, and the efficacy of anti-VEGF therapy.







Comments (0)