This retrospective cohort study adheres to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guideline for cohort studies [23]. The study was approved by the Advocate Aurora Health Institutional Review Board (22.193ET), which waived consent for this retrospective limited dataset and was conducted in accordance with the Helsinki Declaration of 1964. Permission was obtained to access and use data collected from the systems database. RK and NG had full access to all the data in the study and take responsibility for its integrity and the data analysis. Data or other study material are not publicly available due to the nature of the data source (patient electronic health records).
Data Source and Setting
This study was conducted at Advocate Health-Midwest, a large and diverse not-for-profit integrated healthcare organization serving over three million patients and encompassing 27 hospitals, more than 500 outpatient locations, and a clinical laboratory system.
Data were extracted from Epic (Epic, Verona WI), a fully integrated EHR system that contains linked medication history data, including prescription fill data from major pharmacy benefit managers (PBMs) and retail pharmacies connected with the e-prescribing vendor Surescripts (Surescripts, LLC, Arlington, VA). Surescripts returns 12 months of medication history data with every patient visit via the Medication History for Ambulatory interface [24]. Additionally, the health system-owned outpatient pharmacies return detailed pharmacy activity via the integrated outpatient pharmacy module of the EHR.
Study Design, Participants, and Data Collection
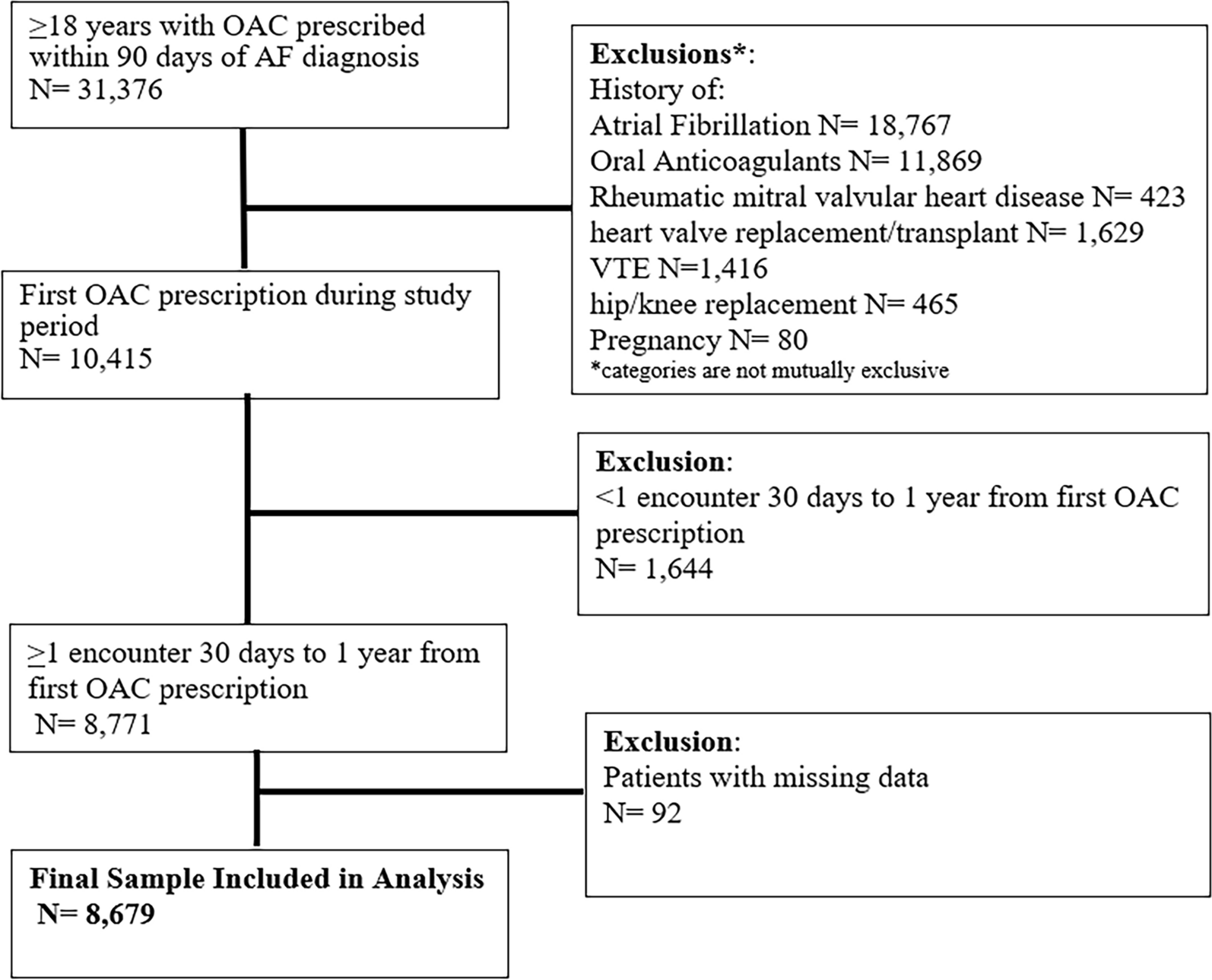
Patient-level data were extracted to identify incident patients with AF newly diagnosed between 2020 to 2021. Data were extracted if patients were ≥ 18 years old, newly diagnosed with AF (International Classification of Diseases [ICD] 10 Codes I48.0–4 and I48.91), received an OAC prescription within 90 days of AF diagnosis, and had at least one encounter with the system between 30 days and 1 year post OAC prescription. Prescriptions were either for direct-acting oral anticoagulants (DOAC: apixaban, rivaroxaban, dabigatran, and edoxaban) or vitamin K antagonists (VKA: warfarin). Data was extracted from the EHR in May 2023. This last criterion was included because a 1-year history of prescription data (used for the adherence measures) was only available and updated if the patient had an encounter with the system after they filled a prescription.
The date of the encounter associated with the OAC prescription was assigned as the index encounter. Patients were excluded if they were pregnant or had a history of OAC prescription within 6 months of the index encounter. Patients were also excluded if they had a history of valvular heart disease or venous thromboembolism (VTE) within 6 months of the index encounter or a total hip replacement (THR) or total knee replacement (TKR) surgery within 6 weeks of the index encounter.
Exposure measures (independent variables) included patient demographic characteristics, SDOH and SDOH proxy characteristics, and patient clinical characteristics and were extracted from the EHR at the index encounter. Demographic characteristics included age (categorized into < 65, 65–74, and ≥ 65 years per CHA2DS2-VASc score categories) [25] and race/ethnicity (categorized into five mutually exclusive groups including white, Black, Hispanic/Latino, Asian, and other [including American Indian or Alaska Native, Native Hawaiian or Pacific Islander, and unknown]; patients who self-reported being Hispanic/Latino were categorized as such, regardless of their race or ethnicity). SDOH and SDOH proxy characteristics included sex, insurance category, employment status, and referral to social work. Clinical characteristics included OAC type (categorized into VKA versus DOAC), treatment setting (categorized into inpatient versus outpatient), provider specialty at prescription, hypertension (defined using ICD 10 codes), CHA2DS2-VASc scores (a modified CHA2DS2-VASc score was calculated by congestive heart failure [+ 1 point], hypertension [+ 1 point], age 65–74 [+ 1 point], age > 75 years [+ 2 points], diabetes [+ 1 point], stroke/transient ischemic attack/thrombotic event [+ 2 points], vascular disease [+ 1 point], and female sex [+ 1 point] for a maximum score of 9 points. Vascular disease is defined as prior myocardial infarction, peripheral arterial disease, or aortic plaque) [25], and HAS-BLED score. A modified HAS-BLED score was calculated using demographics, ICD-10 codes, and medications prescribed; it does not include lab values. The modified HAS-BLED score was calculated as follows: hypertension (+ 1 point), abnormal renal function (+ 1 point), abnormal liver function (+ 1 point), stroke (+ 1 point), bleeding predisposition (+ 1 point), age > 65 years (+ 1 point), alcohol (+ 1 point), and drugs (+ 1 point) for a maximum score of 8 points [25].
Primary outcomes were based on the literature and included primary nonadherence, defined as failure to fill an OAC prescription within 30 days of first OAC prescription [26]; secondary nonadherence, defined as the proportion of days covered of less than 80% over 1 year from first OAC prescription [27]; and nonpersistence, defined as an unsupplied days count that is greater than 30 consecutive days at any time over a 1-year period from first OAC prescription [28]. Primary nonadherence was evaluated among all patients included in the analytic dataset, while secondary nonadherence and persistence were evaluated among a subset of patients who filled an OAC prescription (ever) and had at least one encounter at 1 year or later from their prescription date. Secondary outcomes included all-cause mortality, identified on the basis of discharge disposition, and stroke and bleeding, defined using ICD codes at 1 year from first OAC prescription.
Statistical Analysis
Descriptive statistics were calculated for all variables and presented overall and by primary adherent versus primary nonadherent using mean ± standard deviation (SD) or median (interquartile range, IQR) for continuous variables and count/percentages for categorical variables. All comparisons were made between groups using χ2 tests for categorical data and Student t tests or Mann–Whitney tests as appropriate for continuous data.
A multivariable logistic regression model was built to evaluate the likelihood of primary nonadherence and included a list of potential exposure measures that were identified on the basis of the literature (Table 1) [29]. Backwards elimination was used for covariate selection [29], and the final covariates included in the model are age, sex, race/ethnicity, insurance status, employment status, referral to social work, hypertension, smoking, OAC type, treatment setting, provider specialty at prescription, CHA2DS2-VASc score, and HAS-BLED score. These variables were also evaluated for collinearity as part of covariate selection, and no variables were excluded. Similar multivariable logistic regression analyses were conducted for secondary nonadherence and nonpersistence outcomes. Results from these models are presented as odds ratio (OR) and associated 95% confidence intervals (CI).
Table 1 Baseline characteristics of patients diagnosed with atrial fibrillation and prescribed an OAC between 2020 and 2021Multivariable Cox proportional hazard models were built to evaluate the association between primary nonadherence with clinical outcomes, including the time from prescription to the first bleed, death, and stroke. The same covariates utilized in the logistic regression models were included here. Patients were censored at the time of VTE or TKR/THR during the follow-up timeframe. The hazard ratios (HR) and associated 95% CIs were reported.
All the statistical analyses were completed using SAS software 9.4 (SAS Institute Inc, Cary, NC). All tests were two-tailed, and an effect estimate (OR or HR) with a 95% CI that does not include the null value of 1 was deemed statistically significant.
A missing/unknown category was included when reporting each variable in descriptive analysis. Given very low proportions of missing data from the EHR data used in this study, no imputation of missing values was performed [30]. Any cases missing values on variables in models (e.g., age) were excluded from the analytic sample for that analysis.








Comments (0)