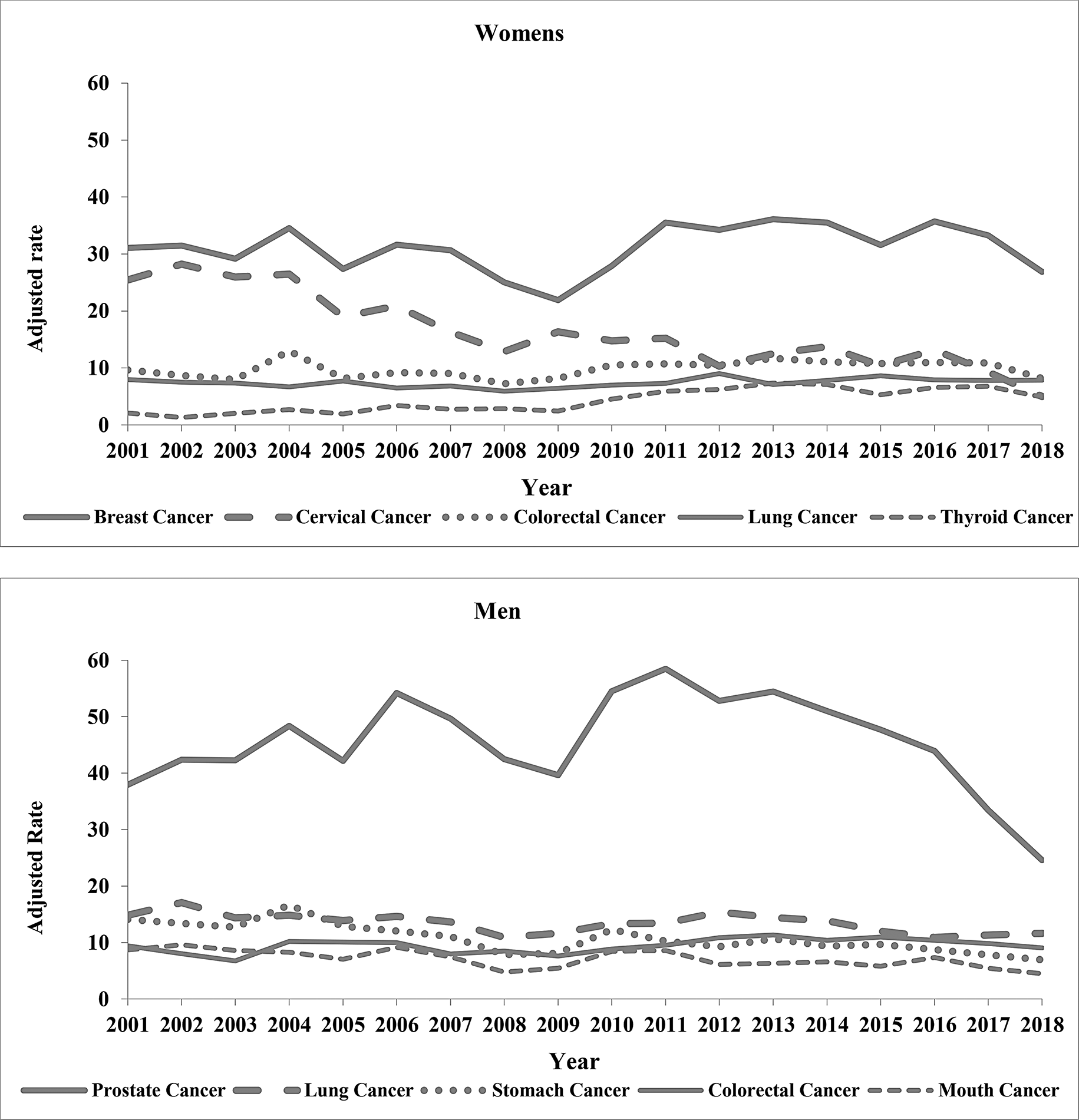
This study presented trends in age-standardized incidence rates of the five most common types of cancer for both sexes in the state of Mato Grosso, as well as the two most common types in men and women, according to health regions, from 2001 to 2018. During this period, the most common cancers in the state, excluding non-melanoma skin cancer, were prostate, breast, lung, colorectal, and cervical cancers. This pattern differs from global and Latin American and Caribbean profiles, where breast and stomach cancers rank as the most and fifth most common, respectively [1]. In the Central-West region, colorectal cancer is estimated to have a higher incidence than lung cancer [2]. However, the cancer profile in Mato Grosso aligns with studies conducted in Goiânia, Goiás, and São Paulo [26, 27]. The highest incidence rates were observed in the North Center, South, Teles Pires, and Middle North health regions.
In men, prostate and lung cancers were the most common, while in women, breast and cervical cancers were the most frequent. The prevalence of prostate and breast cancers is consistent with global and Brazilian patterns. The cancer occurrence profile in Mato Grosso possibly reflects the concept of epidemiological transition, which explains changes in disease patterns due to factors such as infections, socioeconomic development, and unhealthy lifestyle habits [1, 9]. Regarding changes in demographic, socioeconomic and infectious profiles in Brazil and Mato Grosso, several studies point to an epidemiological transition that reflects the process of change in the predominant diseases over time. In particular, Brazil has experienced a significant reduction in mortality from infectious and parasitic diseases, which were dominant in past decades, while chronic non-communicable diseases, such as cancer and cardiovascular diseases, have become more prevalent [28, 29].
In the regional context, Mato Grosso state reflects these changes, but with a transition that occurs unevenly between regions. The study of the epidemiological profile in Brazil showed that while the southern and southeastern regions experience a higher prevalence of chronic diseases, the North and Midwest regions, including Mato Grosso, still face challenges related to infectious and parasitic diseases [30]. Given that agribusiness is the main economic driver in the state, this industry likely influences the cancer occurrence profile [31].
The great regional variability in the occurrence of cancer cases over the period studied deserves to be highlighted. This situation is possibly due to the fact that, in each health region, the health system works in different ways, and the diagnostic network is concentrated in municipalities with higher density, thus influencing the quality of the data recorded [32].
The variability observed in the Garças Araguaia region for prostate cancer is a good example. This situation is due to the large difference in the number of cases observed in the first two and last two years of the study period in relation to the other years. Possibly, three factors justify this situation, namely: the RCBP was implemented in Mato Grosso in 1999 and the registration of cases did not yet occur properly in the initial years; the closure in 2016 of a state reference Health Unit for cancer care; and the state service responsible for Cancer Surveillance did not carry out an active search for cases in the last two years of the study period. However, the possibility of underreporting cannot be disregarded.
The quality indicators used to assess the RCBP data are closely related to the number of cases and the availability of health services for cancer diagnosis and treatment within the registry’s coverage area [33]. The IARC evaluates the quality of RCBP databases, but the CI5 XII (IARC) publication currently classifies these databases based on information quality without specifying exact values for quality indicators [33, 34]. In low- and middle-income countries (LMICs), these indicators pose challenges due to incomplete data, the need for active case finding, and the sustainability of registries to monitor cancer rates and trends over the long term. Despite not meeting all quality control standards, the dissemination and analysis of cancer registry information remain valuable. They can provide insights into healthcare system deficiencies and support planning for cancer control actions [9, 22, 33].
Regarding the quality of RCBP data, this study found that data quality indicators for primary tumor sites were generally better for females, with %MV above 70.0% observed in four of the five most common cancers in women and %DCO below 12.0% in three. However, the %DCO for lung and stomach cancers was notably higher compared to a study conducted in Mendoza, Argentina [35] Tracking cases reported through death certificates could be a way to improve data quality by reducing %DCO.
An important differential of the State in relation to other Brazilian states is in the territorial extension and vigor of the economy based on agricultural production. The health regions are very distinct demographically, socially, economically and in the structure and access to the health service network for cancer care. In health regions that have a predominance of chemical agricultural production dependent on agribusiness, there is evidence of high exposure to carcinogenic agents and ineffective performance of cancer surveillance services.
In analyzing cancer incidence by health region, the highest age-adjusted rates were concentrated in the four most developed, populous, and socioeconomically advanced health regions, which represent 57.0% of the state’s population. Mato Grosso showed an increasing trend for prostate cancer between 2001 and 2013 (APC: 2.6%), with significant increases in specific regions such as Garças Araguaia (2001–2003 and 2003–2016), Southwest, Middle North (2001–2015), and South (2001–2006). Conversely, decreasing trends were observed in the Baixada Cuiabana, Garças Araguaia (2016–2018), Southwest (2015–2018), and South (2012–2018) regions. A similar reduction was noted in Cuiabá and Várzea Grande (2006–2016) [37]. In Brazil, an increasing trend was observed from 2001 to 2016 (AAPC: 0.47). A global study on prostate cancer incidence from 2000 to 2019 found increases in 73.0% of countries, stability in 28.1%, and decreases in 10.1%, with the highest rates in countries with a high or very high Human Development Index (HDI) [7, 38]. The rise in prostate cancer incidence may be attributed to advances in diagnostic methods, improvements in data quality, increased life expectancy [39], modifiable risk factors related to environmental and lifestyle factors such as diet and physical activity, non-modifiable factors such as age, hormonal aspects, and genetics [1], challenges in accessing healthcare, local screening and diagnostic practices, and differences in therapeutic approaches and care quality [40,41,42,43]. Men in low socioeconomic settings may face higher risks compared to those in other settings [41]. Conversely, the decrease or stabilization in incidence may reflect a reduction in screening due to a lack of promotion for the prostate-specific antigen (PSA) test by some health agencies [44]. The non-recommendation by the Brazilian Ministry of Health is due to the lack of scientific evidence so far that this practice brings more benefits than risks, as well as, there is no evidence that PSA screening reduces overall mortality for men of any age and consistent evidence that screening and active treatment lead to harm [45]. Despite the utilization of digital rectal examination (DRE) in clinical practice to detect prostate cancer, there is currently no evidence indicating that DRE alone or in conjunction with the PSA test results in a reduction in prostate cancer mortality [46]. To increase this proportion, it is essential to improve awareness of men’s health and the importance of screening, as well as to ensure that health services are accessible and appropriate to the needs of this population.
Although lung cancer is the most common cancer in men worldwide, its incidence has been declining globally and in Brazil since the 1980s. It is estimated to be the third most common cancer in men in the Central-West region in 2023 and to account for 30.0% of all cancers in men in Mato Grosso [2]. This study found a decreasing trend in lung cancer incidence in men from 2001 to 2009 (APC: -4.2) and 2012–2018 (APC: -5.9), with reductions also observed in the Baixada Cuiabana (AAPC: -2.4) and Garças Araguaia (AAPC: -3.8) regions. Similar findings were observed in studies conducted in the Greater Cuiabá area (AAPC: -2.2) [37, 47]. Despite this trend, eight health regions, representing 78.2% of the state’s population, had incidence rates during the study period that exceeded the estimated rate for the state in 2023 (11.98/100,000 men) [2]. Key factors contributing to this trend include reductions in smoking and exposure to secondhand smoke, as approximately 85.0% of diagnosed cases are associated with tobacco use [48]. Brazil’s tobacco control policies, focusing on legislative and social changes, have effectively contributed to smoking cessation rates [49]. According to the National Health Survey (PNS), in Brazil, there was a reduction in the prevalence of adult male smokers from 18.9% in 2013 to 15.9% in 2019 [50], and in 2023, this percentage was 10.2% [51], while the WHO Global Report on Trends in the Prevalence of Tobacco Use 2000–2025, points out that in 2020, 36.7% of the adult population in the world used tobacco.
Additionally, occupational and environmental exposure to carcinogenic agents, particularly in an agriculturally chemical-dependent economy, plays a significant role.A prevalence study of occupational and environmental exposures among patients in Mato Grosso found pesticides to be the most common exposure, affecting around 20.0% of patients [36]. Despite the decreasing trend found, the absence of planned and systemic interventions by state public management since the early 2010s remains a concern.
Even though, female breast cancer has surpassed lung cancer as the most diagnosed cancer worldwide, excluding non-melanoma skin cancer, the trend in Mato Grosso showed a decrease from 2001 to 2009 (APC: -3.6) with an increase in the Southwest and Araguaia Xingu regions (AAPC: 5.8). This state-level trend aligns with observations from developed countries since the 2000s [1]. However, a shorter historical analysis found an increasing trend from 2009 to 2016 in the state and a decreasing trend in Baixada Cuiabana from 2000 to 2009 [7]. Since the 2000s, increasing breast cancer incidence has been noted in developing countries, including South America, Asia, and Africa [1]. The rise in incidence is linked to aging, behavioral, environmental, and reproductive risk factors, as well as economic development, improved healthcare services, and enhanced early detection through widespread mammographic screening, recommended in Brazil for women aged 50 to 69 years [1, 52]. Notable behavioral risks include alcohol consumption, overweight, physical inactivity, and exposure to ionizing radiation [53,54,55]. Among reproductive factors, fewer children, shorter periods of exclusive breastfeeding, and delayed childbirth are significant [1]. Regarding the availability of services and improvements in early detection, a study conducted in São Paulo and Campinas (Brazil) found a statistically significant association between suspected breast cancer identified by Primary Health Care (PHC) and economic and cancer care variables, such as breast examination at PHC before referral to Specialized Care (SC), initial mammogram requests by PHC, and continuity of care in PHC post-treatment [56].
A global trend study found increasing rates of cancers associated with socioeconomic development, such as breast and lung cancer, particularly in low- and middle-income countries [57]. Studies conducted in the Barretos region and São Paulo districts support this association, as breast cancer incidence rates in São Paulo were 30% higher than in Barretos, particularly in districts with high socioeconomic levels [12]. The varying trends in breast cancer incidence across regions may reflect differences in exposure to risk factors, the availability and access to healthcare services, and the differing use of early detection procedures [56, 58, 59]. Although this study did not identify statistical significance for the trend in breast cancer incidence in the state from 2009 to 2018, the ratio of mammograms in women aged 50 to 69 years has always been lower than that of the Central-West region and the country. This ratio in the state in 2021 was the same as in 2008 (0.08) [60]. These results demonstrate great weakness in the actions for early detection of this cancer, calling into question whether the downward trend detected in the period from 2001 to 2009 is due to the secondary prevention actions implemented.
Globally, cervical cancer is the fourth most common cancer among women, and the third most common in Brazil and the Central-West region [2, 61]. In Mato Grosso, it is the second most common, excluding non-melanoma skin cancer. The study identified a decreasing trend in cervical cancer across the state and in the nine health regions with calculable rates: Baixada Cuiabana, Garças Araguaia, West, North Central, Northwest, Vale do Peixoto, South, Teles Pires, and Middle North. A decreasing trend has been observed in recent decades in studies conducted globally and in Brazil. Notable reductions have been found in Latin America, Asia, and Brazilian cities such as Belém, Palmas, Salvador, Fortaleza, Distrito Federal, Belo Horizonte, Grande Vitória, Curitiba, São Paulo, Porto Alegre, Campinas, and Goiânia [62, 63]. A different situation, particularly among young women, has been observed in some countries in Eastern Europe, Asia, and Central Europe. The highest incidences have been reported in Sub-Saharan African and Southeast Asian countries [64, 65]. Although the main risk factor for cervical cancer is persistent infection with an oncogenic type of Human Papillomavirus (HPV), factors related to immunity and genetics can influence the mechanisms that determine the persistence or regression of the infection, as well as associated cofactors such as age, smoking, education, and multiparity [48, 66]. The incidence of this cancer can be reduced through vaccination against oncogenic HPV types, screening through cytopathological examination, and treatment of precursor lesions in women aged 25 to 64 years [48]. The Supplementary Information (SI-5) presents in a systematized way the primary and secondary prevention measures by type of cancer.
Despite recent reductions in cervical cancer incidence in Brazil and Mato Grosso, HPV vaccination coverage has declined, and the ratio of cytopathological exams to the female population aged 25 to 64 years has decreased. In 2019, 87.08% of Brazilian girls aged 9 to 14 received the first vaccine dose, dropping to 75.81% in 2022. Coverage among boys fell from 61.55% in 2019 to 52.16% in 2022 [67]. The ratio of cytopathological exams to one-third of the female population decreased from 0.56 in 2008 to 0.29 in 2021 [60].
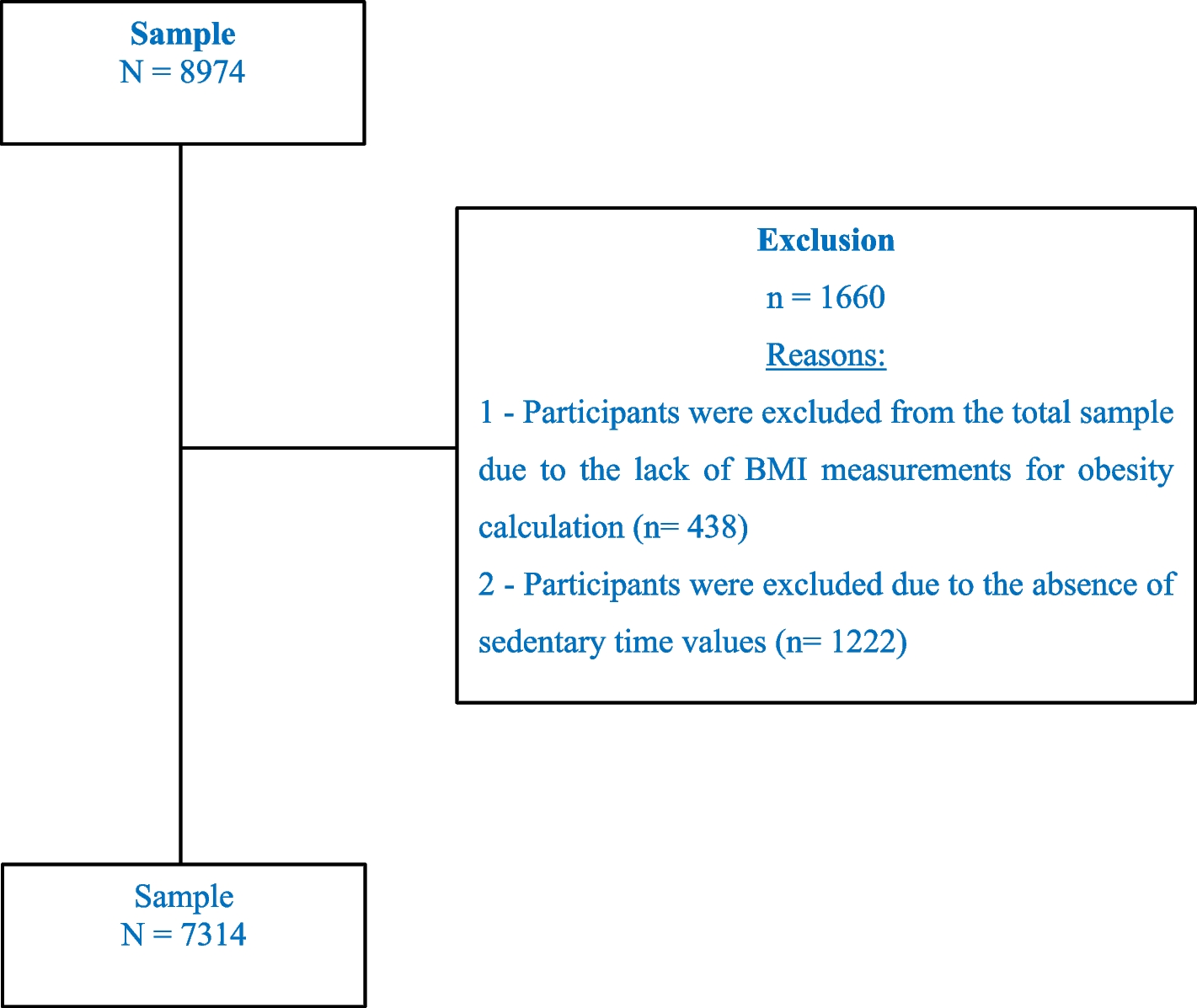
The limitations of the present study include the possibility of underreporting, filling and coding errors, and the incompleteness of certain variables, which may have impacted the analysis and interpretation of the results. If cancer cases over the observed period were constant, it would be possible to obtain a more detailed view of the variations in incidence rates. However, this was not observed, because there is regional variability and, in some periods, there were no cases of cancer to be analyzed, so it was not possible to apply the method. Although this study identified temporal associations, it was not possible to identify causality because underlying factors can influence both exposure and outcome, and in the trends identified it was not possible to assess the influence of seasonal or socioeconomic changes. Nevertheless, the study stands out as one of the first to analyze trends in the incidence rates of the most frequent cancers in both sexes in Mato Grosso, identifying significant regional variations. Additionally, it highlights the local epidemiological profile, reflecting the epidemiological transition and the relationship between socioeconomic development and the prevalence of cancers associated with infections and unhealthy lifestyle habits. Furthermore, the analysis of data quality revealed better completeness for female cancers, which is useful for identifying healthcare system deficiencies and guiding control action planning, particularly in regions with higher rates.





Comments (0)