
Remember me




For this study, we included patients who were hospitalized at the University Hospital of Basel between February and September 2023 and were eligible to participate in the study. Patients were hospitalized in two wards of the department of General Internal Medicine. All patients included were required to provide their written informed consent, which was documented by the participants’ signature. This study was approved by the local cantonal Ethics committee.
Inclusion criteria were age > 18 years and a planned in-hospital-stay of > 24 h. Exclusion criteria were inability to sign written informed consent, significant mental or cognitive impairment as well as medical reasons making it impossible to wear the device, such as allergic reactions, wounds, amputations, excessive hairiness impairing signal quality, edema, installed venous access and others. Baseline data include age, gender, weight and height. Patients with known hypercapnic respiratory failure were analyzed separately to take their lower SpO2-limits (88–92%) into account. Patients skin tone was assessed using Fitzpatrick’s scale [1,2,3,4,5,6]. Hairiness at the location of the device was graded from 1 – 3 (1 = mild, 2 = moderate, 3 = excessive). In patients with severe body hair, signal quality was checked, and if it led to insufficient data quality, the patients were excluded from further analysis.
For this study, we used the Corsano CardioWatch 287–1, a clinically validated, CE-marked and certified class IIa medical device, which measures heart rate and respiratory rate. More information about the device can be found here: https://corsano.com/wp-content/uploads/2021/04/Corsano-287-1-Leaflet.pdf. Wearable data was collected using the Device Hub IoMT platform developed by the Swiss-based company Leitwert®. Further data was extracted from the clinical information system MEONA®. Due to a missing interface to MEONA we did have to calculate the NEWS2 retrospectively for this trial.
For conventional measurements the Welch Allyn Connex Spot Monitor (Welch Allyn Canada Ltd) was used by nurses. Measurements included an automated oscillometric blood pressure machine using the arm and core temperature using an Ear Thermometer. Oxygen saturation, heart rate and respiratory rate was derived from a Masimo pulse oximetry sensor.
In this trial, while five of the seven parameters required for calculating the NEWS2 score can be measured by wearable devices, none of the currently available devices covered all parameters satisfactorily. Specifically, respiratory rate was measured using wearables, but the accuracy was insufficient for our needs. Although oxygen saturation can be measured by wearables, it was assessed using a separate device (Welch Allyn), as the sensor used in the trial did not capture this parameter. The need for oxygen therapy was recorded manually in the electronic medical record (EMR) by nursing staff when oxygen was provided, eliminating the need for a wearable to track this information. Heart rate was successfully measured with wearable sensors and included in the trial. Although blood pressure can be monitored by wearables, it was measured using a separate device (Welch Allyn) since the trial sensor lacked this capability [12]. Level of consciousness could potentially be integrated into wearables by prompting specific reactions from patients, but this feature is not yet available. Finally, while core body temperature can be tracked by wearables, it was measured with a separate device (Welch Allyn) during the trial due to the wearable sensor’s limitations [13].
Study proceduresAfter giving written informed consent, patients were handed a wristband with a PPG-sensor, that was put on the wrist. Participants were instructed to wear the device continuously for three days. Following this timeframe, patients were then asked whether they had worn the device regularly, and if not, to state reasons for that. Furthermore, a semi structured questionnaire was given to ask patients about their experiences with the device. The data collected via the wearable was solely observational and was unavailable to clinical professionals during the study. It had no clinical impact on patient treatment, as all patients received standard medical care.
Data collection and analysisAll data collected for the analysis of this study was coded by a unique patient ID. Using a distinct device ID, the wearables were linked to the Bluetooth-to-Wifi gateways, which were integrated with the secure hospital network and controlled by the Device Hub IoMT platform. Raw and processed data was transmitted continuously with Transport Layer Security (TLS) encryption to an in-house database, where it was stored. Under consideration of the typical range of Bluetooth Low Energy connections, the gateways for data transfer needed to be placed in the same rooms as the participants. The Device Hub used in the study allowed to control device status, data availability and signal quality of the wearables. Irregularities, such as poor data quality or missing data were checked regularly by study personnel via the Device Hub user interface. If needed, a check-up was made to detect technical issues or whether the device was not worn by the participants during that time.
At time of patient discharge, NEWS2-Values were calculated and noted in the electronic Case Report Form (eCRF). Data were derived from available measurements in the electronic health record (EHR) and comprised information routinely collected by nurses using standard clinical devices, encompassing all six parameters necessary for NEWS2-calculation. Data were attached with timestamps of measurement.
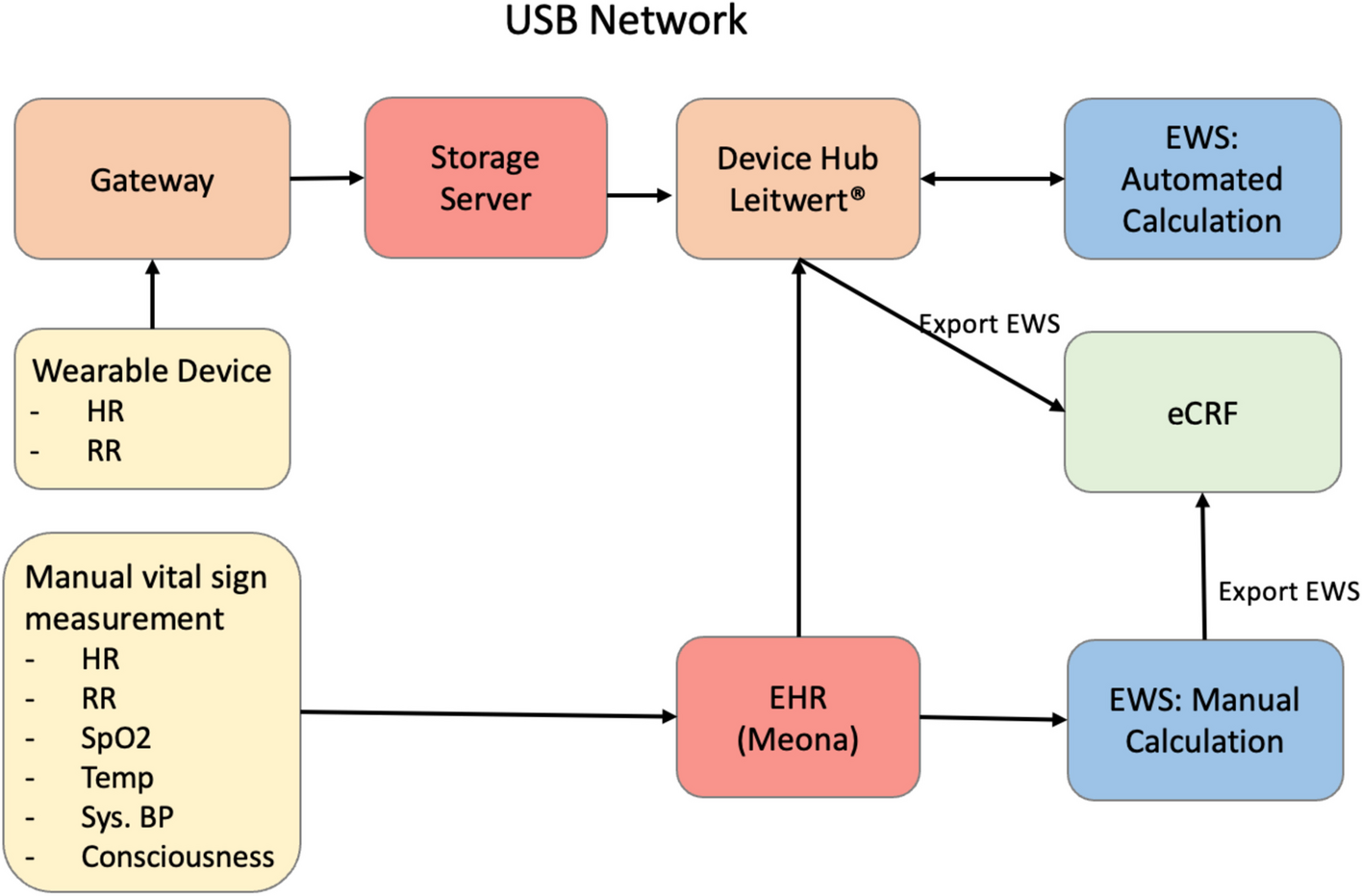
Retrospectively, NEWS2 was calculated conventionally with data solely from the EHR and automatically, where NEWS2 was calculated using data from the wearable device (heart rate, respiratory rate) combined with data from EHR (systolic blood pressure, temperature, blood oxygen saturation, consciousness). Data collected by the wearable device was paired with the data documented in the EHR based on timestamps and data quality. To assess for interrater variability between both methods, we used Cohen’s Kappa analysis [14, 15]. Figure 1 details the process of data collection and processing.
Fig. 1
Flowchart showing data measurement and processing. Data acquired by the wearable were combined with conventional measurements stored in the hospitals EHR for further NEWS2-calculation, also conventional measurements stored in the EHR (= Meona) were used for NEWS2-calculation. The final measurements were reported to the eCRF. Abbreviations: eCRF: electronic Case Report Form; EHR: Electronic Health Record; HR: Heart Rate; RR: Respiratory Rate; Temp: Body Temperature; Sys. BP: Systolic blood pressure
If a participant decided to withdraw consent, data which had already been collected was included into the analysis, provided that the participant agreed with its use.
Participant questionnaireAfter participants had ended the study, a semi structured questionnaire was performed. They were questioned whether they’ve had any prior experience with such wearable devices. Also, they were asked whether they had worn the device regularly and if not, we asked for their reasons. Participants were asked whether they had experienced any difficulties wearing the device and if so, to specify those difficulties. Furthermore, they were questioned about their technical proficiency on a scale between 1 (very good) and 5 (not good at all). Using the same scale, participants were asked on their opinion of continuous monitoring in hospitals, and how safe they would feel if their vital signs were continuously monitored by the device (1 = very safe, 5 = not safe at all). We asked the participants, if they would use such a device at home if it was prescribed to them by their doctor and if not for specific reasons behind it. Lastly, they were asked what they thought potential benefits of wearing such a device could be, but also what concerns they had about such devices. Additionally, we asked them whether they had any further suggestions or comments about the use of such devices in the hospital.
Comments (0)