
Remember me






This is the first case report to describe breast and nipple pain caused by a hard, removable object obstructing the nipple orifice in two lactating people. We suspect that there is a spectrum of disease presentation: milk blebs and stones lie on a continuum. Repeat trauma from the breast pump, infant latch, or manual manipulation results in a pathological inflammatory response at ductal opening that triggers a cascade of events eventually leading to fibrosis with or without stone formation. While the patient in case 1 engaged in some significant nipple manipulation, the patient in case 2 did not, suggesting manipulation is not the only source of this particular breast pathology. Nevertheless, patients should be advised against manual manipulation of white spots on their nipple to avoid additional trauma and worsening of their condition. Milk blebs treatment has been outlined elsewhere [2,3,4,5]. Both patients had a similar clinical presentation to those described in the online fora consisting of nipple trauma from latch and/or breast pump use, hyperlactation, and nipple and breast pain relieved after stone removal. Likewise, both of our patients and several patients in online fora have described not being able to remove the stones without painful manipulation, suggesting that the advice to not manipulate the breast may be hard to follow.
Breast calcifications are known to occur throughout the lifespan and may represent benign or cancerous lesions in the breast, but these calcifications are predominantly composed of calcium oxalate and calcium phosphate, with mineralogical differences between malignant and benign lesions poorly understood [9]. The Ca:P, Mg:Ca, and Na:Ca ratios of the stones were different from those reported for breast calcifications [9], suggesting breast calcification is unlikely to be the etiology for the obstructing objects experienced by our patients.
Objects obstructing milk ducts, called “lactoliths,” have been described in the veterinary medicine and dairy science literature, but their composition and etiology has not been defined [10, 11]. What has been described are proximal and internal teat canal obstructions, which are thought to contribute to stone formation. There is, of course, a difference in the diameter and length between the cow teat canal and human nipple ducts, which limits our ability to translate what is known about stone formation in the cow teat canal to the human experience. A major anatomical difference between the teat and the nipple is that, by definition, a teat only has one galactophore (milk duct) while the nipple has two or more. The diameter of all galactophores is smallest at its orifice, progressively increasing until it reaches the cistern (in cows) or the nipple base (in humans).
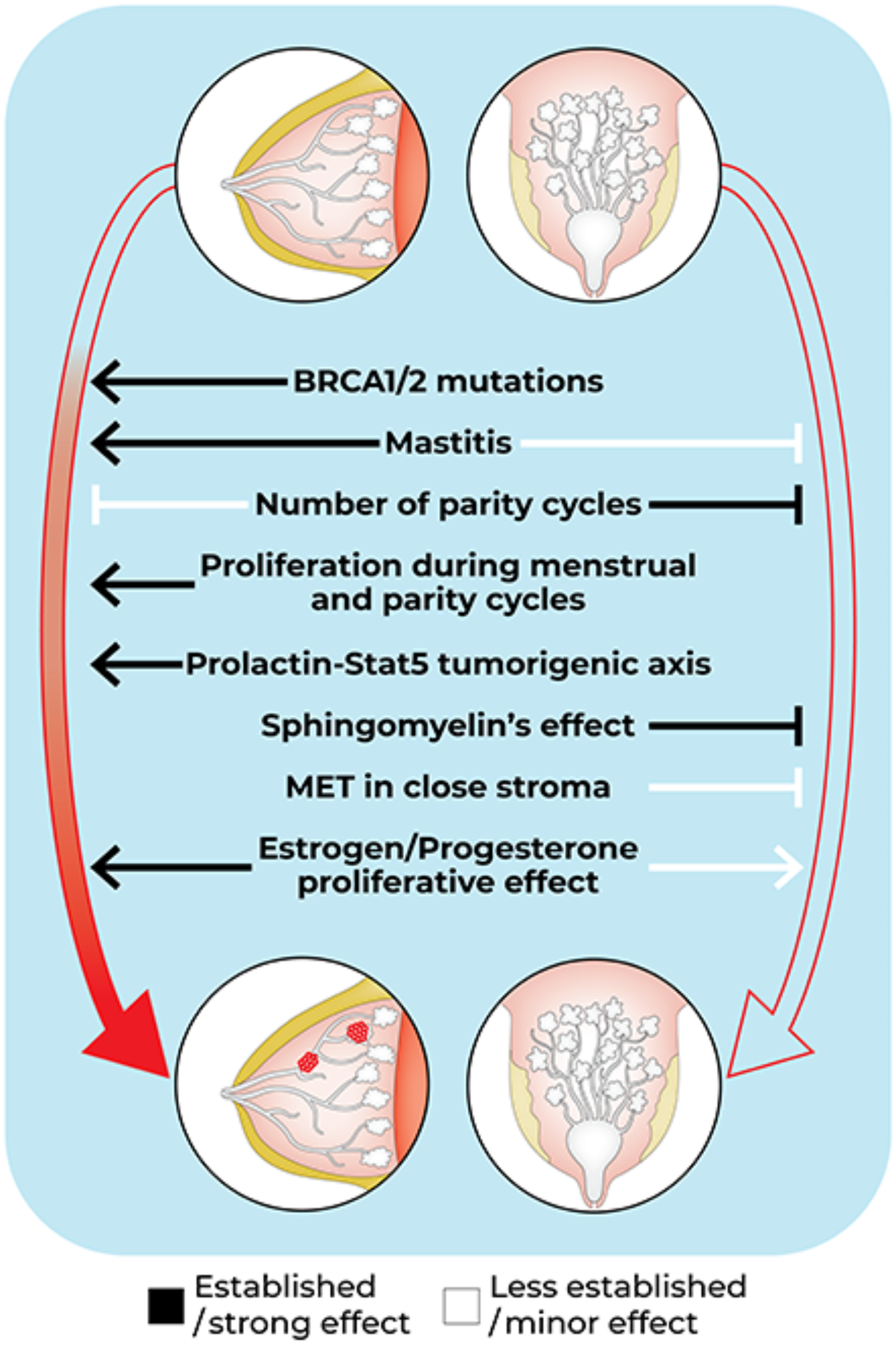
Since the mammary gland is a tubulo-acinar exocrine gland that shares many similarities with other glandular structures, we also sought to find examples in other exocrine glands of ductal obstructions where the duct is comparable in diameter and length to the human nipple. We found numerous reports of painful obstructions of lacrimal (dacryoliths) and salivary (sialoliths) ducts and glandular structures, which, akin to the mammary gland, secrete a fluid that then traverses a long, small duct before expulsion. Using the literature on teat obstructions in dairy cows and dacryolith and sialolith formation as a framework, we have developed three potential mechanisms by which an obstructing object in the human nipple duct may form (Fig. 3): (1) nipple orifice irritation, trauma, or obstruction, (2) nipple duct inflammation, fibrosis, stricture, or other anatomic defect, and (3) factors deep within the mammary tree that promote stone formation in the human nipple duct.
Fig. 3
Proposed mechanisms of ductal stone formation. The primary insult leading to stone formation is likely due to external trauma (A) at the ductal orifice. In humans, there are numerous causes of nipple apex trauma, from a latch problem to breast pump use or topical agents that cause microtrauma, inflammation, and thickening of the skin at the ductal orifice (B). Internal ductule trauma or malformation (not shown in figure) likely co-exists with injury at the orifice. In dairy cows, teat hyperkeratosis damages the anti-microbial barrier, resulting in microbial dysbiosis (C) in the teat canal. Likewise, high vacuum, especially when “dry milking” before stimulating a let down, is associated with mucosal avulsion within the teat canal, and can lead to stricture of the teat canal. Finally, some individuals may be prone to stone formation based on the composition of their breast milk, milk microbiota, or diet (D). While less likely, it is possible that some individuals have a congenital anomaly in their milk ducts (not shown in figure) such that there is an increased likelihood of milk stasis with or without the translocation of microbes from the skin surface, resulting in stone formation
External Trauma at the Ductal OrificeWe believe that external trauma to the ductal orifice is an important factor in the development of an obstructing object in the duct. Both of the patients in this case series had grossly intact nipples on physical exam, but had experienced nipple trauma from latching an infant with ankyloglossia. We cannot exclude the possibility that nipple skin was additionally irritated by manipulation with forceps during stone removal (Case 1), breast pump use, new topical agents, nursing pads, or bras that were used in the postpartum period, resulting in inflammation of the skin at the nipple orifice (Fig. 3). Consistent with this latter concern was the presentation of Case 1 with a nipple “bleb,” typically thought to represent hyperkeratotic obstruction of an inflamed nipple duct orifice [4]. Teat obstruction in dairy cows is almost always trauma-related (> 90%) and not due to a congenital anatomic defect in the teat canal itself [10, 11]. External factors, including high vacuum from the milk claw and topical irritants, are known to cause fibrous remodeling, epithelial metaplasia, and loss of specialized blood vessels resulting in complete scarring over of a teat opening (teat hyperkeratosis, akin to a milk “bleb” in humans) or nonfunctioning downstream segments of a nasolacrimal ductule, respectively. Human nipples are especially prone to external insults during the lactation experience, as single, small ducts branch and coalesce multiple times within the human nipple, unlike in dairy cows (Fig. 4) [12]. Several tiny ductules open to one orifice at the nipple apex (Fig. 4), or one ductule leaves a cluster of ducts to join a new one at a different orifice [12]. Therefore, if one ductal orifice is blocked, there can be deleterious downstream effects on numerous, seemingly unpredictable ducts and segments of the mammary gland.
Fig. 4
Adapted from Rusby et al. [12]
A simplified cartoon showcasing variations in the microanatomy of ducts in the human nipple. Larger ducts from the mammary gland come together at a “waist” at the level of the nipple base. On the nipple apex, there are numerous crevices where one or more ductal openings exist. As the ducts travel through the nipple towards its apex, they can end in a blind pouch (A), exit the nipple through an orifice as a single ductal opening (B) or with other ductules (C and D), or, potentially, change routes and leave their “bundle” to join a different group at an orifice (D to C), although this last situation is less likely based on what is known about mammary embryology. Likewise, there are other ducts and sebaceous glands that are not milk-secreting located in the nipple (E).
Internal Ductule Trauma or MalformationThe presence of a blockage at the level of the ductal orifice may not directly translate to the formation of a stone in the nipple duct. It is likely that a secondary hit (e.g., two-hit hypothesis) is required, such as damage to internal ductal structures, although, in cows, severe teat hyperkeratosis is thought to be associated with the development of mastitis in that quarter [13]. The teat canal, and possibly the nipple duct, can also be damaged by the vacuum if it is turned on before milk let down occurs. If there is no milk flowing from the udder to the teat canal, as would occur after let-down, the walls of the teat canal collapse, thereby subjecting the fragile epithelium lining the teat canal to further damage, resulting in mucosal avulsion with the possibility of hematoma formation; repeated injury can result in teat canal stricture and loss of that udder quarter [13]. The same may be true for women using the breast pump frequently, not allowing their breast tissue to recover in between pumping sessions, resulting in repeated microtrauma within nipple ductules, which can present as bloody milk with or without blood clots. Once the inflammatory or constricted environment is created, an obstructing object in the duct could begin to form.
A congenital abnormality in the ductule itself may also be responsible for promoting an stone-forming environment. In the example of the dacryolith, its composition was strongly correlated to whether it was formed in the lacrimal sac versus the canaliculus, where concretions devoid of cells (i.e., non-infectious origins) were found exclusively within the lacrimal sac [14]. There is also evidence that an abnormality in a valve of Hasner–a fold of the mucous membrane at the end of a nasolacrimal duct that prevents air from entering the lacrimal sac from the nose–is associated with dacryolithiasis [14]. It is possible that the patients in our case report had something unusual about the anatomy of their milk duct–its circumference, length, tortuosity–that increased the likelihood of stone formation.
Milk Composition and MicrobiotaThe third and final ingredient in the recipe of stone formation is likely the milk composition and microbial community. In recent years, it was discovered that the innermost core of the sialolith is composed of bacteria [15]. It was hypothesized that the biofilm produced by bacteria (e.g., Streptococcus spp.) attracts calcium carbonates and calcium phosphates from the saliva, resulting in mineralization and concretion formation [15]. It is well-known that breast milk and nipple skin contains a multitude of bacterial and fungal organisms, which vary based on a number of maternal characteristics [16, 17]. The same is true in the dairy cows, for whom we have additional evidence that there are three distinct bacterial communities in the teat end apex, teat canal, and milk [18, 19]; it is not known whether the same differential occurs in human mammary tree. Milk acts as a potent selective medium that precludes the growth of specific bacterial lineages; once there is teat apex inflammation, internal canal stricture or trauma, or a change in the milk composition, the microbial communities are perturbed and the result is often mastitis and, possibly for some individuals, stone formation. As we highlighted earlier, the dairy cows’ environment and teat anatomy differs from that of the human, yet they remain superior to many other animal models for hypothesis generation of how microbial communities might impact human nipple stone formation. Their utility has become especially salient as they (alongside goats and a few other livestock dairy animals) are the only other mammals besides humans for whom vacuum pumps are used to regularly remove milk, thereby serving as an elegant animal model for the effects of the breast pump on nipples/teats, milk composition and volume, and animal health.
It is possible that our patients’ breast milk composition primed stone formation (Fig. 3). For example, saliva, urine, and tear composition, respectively, can affect lithiasis. Patients with and without frequent dacryoliths have differences in tear composition, where those with chronic dacryoliths have lower lysozyme and potassium levels, but similar calcium levels to healthy controls [14, 20]. It is thought that low lysozyme levels reduce proteolysis and may create a permissive environment for lithiasis. Sialoliths are composed of proteins at their core and surrounded by inorganic molecules. In one study, lysozyme (95%), lactoferrin (85%) and secretory immunoglobulin A (s-IgA) (75%) were found in nearly all of the submandibular sialoliths [21]. Given that lactoferrin, lysozyme, and s-IgA are also found in high concentrations in breast milk, it would be important to understand how breast milk composition affects stone composition, a patient’s predisposition for stone formation, and the associated symptomatology.
Parental Diet and Water IntakeDiet has been shown to increase the risk of subclincial and clinical mastitis in humans and dairy cows due to the creation of a pro-inflammatory milieu [22,23,24,25]. Our patient in case 1 experimented with elimination of various foods, tracking their intake with a food diary, and measuring serum Ca. At this time, we do not have sufficient evidence to implicate maternal diet in the formation of stones. Our patients reported an improvement in symptoms with adequate water intake. While adequate water intake is important for prevention of nephrolithiasis, it is not known whether the pathophysiology of nephrolithiasis is similar to that of stones in the milk ducts [26]. In the kidney, stones form by a process called nucleation, whereby initial crystal seeds form when ions/molecules cluster together in the nephron or renal calyces. Nucleation of kidney stones is secondary to an altered urine pH, concentration of stone-forming substances, and presence/absence of inhibitory compounds—this process is similar in concept to what we have proposed for stone formation in the nipple duct. Both of the patients in this case report described an inverse relationship between water intake and stone formation, but prospective clinical trials are needed to better understand the relationship between maternal diet and water intake and the milk bleb-stone spectrum of conditions.
LimitationsSeveral important limitations should be considered when interpreting these findings. Most important is that with only two patients, our ability to generalize these findings is limited. While we performed mineral analysis on the stones, we were unable to conduct comprehensive structural analysis, microscopy, or bacterial culture or DNA sequencing of the specimens. Likewise, complete milk samples and compositional analyses were only available from one patient, limiting comparative analyses. We cannot fully exclude the role of mental health factors, including obsessive-compulsive behaviors, that may have contributed to recurrence through repeated manipulation and trauma of the nipple tissue, especially in Case 1. Finally, our long-term follow-up was limited, as one patient was lost to follow-up and the other experienced only one additional occurrence before weaning at 18 months, preventing us from fully understanding the natural history of stone formation and its impact on breastfeeding outcomes.
Recommendations for Future ResearchWe recommend a prospective case series of patients presenting with obstructing objects in their nipple ducts. If a patient has recurrent stone formation, it would be ideal to collect the data described below for each event, and determine inter- and intra-patient variability of nipple anatomy, micro/mycobiome, and stone composition. We do not recommend ductoscopy, as this is an invasive procedure that has low sensitivity and specificity given the small diameter of ductules at the nipple orifice and the numerous pathways a ductule can take from the nipple apex to base [12].
1)Complete lactation history, with aspecial focus on signs and symptoms of nipple trauma, including:
a)breastfeeding practices, pump use.
b)topical and oral medication or agents, type of bra and nursing pads or other items in contact with nipple skin.
c)infant anatomy and latch characteristics.
d)Mental health history, including obsessive-compulsive behaviors.
2)Imaging, including:
a)Dermatoscopic image of the nipple apex.
b)Non-invasive optical biopsy of the nipple orifice to define the histology of the nipple epidermis surrounding the ductal orifice with reflectance confocal microscopy [27], optical coherence tomography, quantitative oblique back illumination microscopy [28], or similar non-invasive optical biopsy method.
3)Stone characterization and analysis, including:
a)Macroscopic/magnified photography of the removed stone.
b)Composition analysis of the stone, including mineral, protein, carbohydrate, lipids.
4)Microbial analysis, including:
a)16s rRNA and ITS sequencing of the microbial communities of stone, milk, and nipple skin using minimally-invasive techniques such as microprojection arrays and swabs. Tissue stripping may be painful [29].
b)Bacterial and fungal culture of milk and nipple skin.
Comments (0)