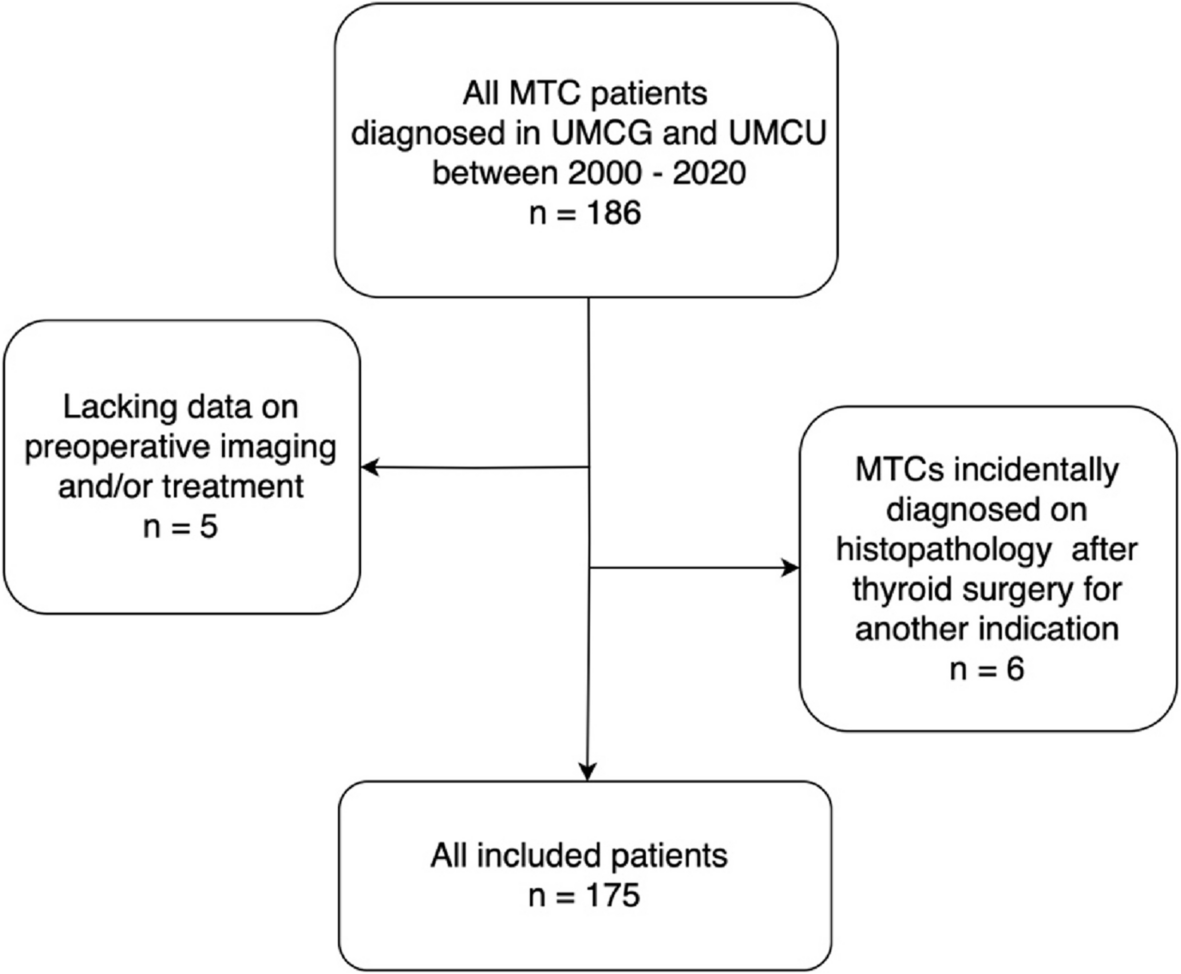
As the technique and quality of PET/CT imaging improves over time, knowing its value in the initial assessment of MTC patients could optimize stratification and treatment at diagnosis. In this two-center, retrospective study of 175 MTC patients, 35 18F-FDG PET/CTs, 33 18F-DOPA PET/CTs, 91 ultrasounds, 33 MRIs and 31 CTs were performed at diagnosis. Both PET/CT scans were superior to ultrasonography, CT and MRI in identifying lateral neck LNMs, with sensitivity rates of 89% and 81% and specificity rates of 100% and 100% for 18F-FDG PET/CT and 18F-DOPA PET/CT, respectively. For the central compartment LNMs, CT was superior, with a sensitivity of 93% compared to 72% on 18F-FDG PET/CT and 39% on 18F-DOPA PET/CT. While CT may therefore be the most optimal modality for identifying central LNMs, the high accuracy for lateral LNMs on preoperative PET/CT, as well as its ability to detect distant metastatic disease, may allow more optimal staging at diagnosis and de-escalation of the initial surgical strategy.
Literature on the role of PET/CT imaging in the preoperative process of MTC patients is very limited, which is highlighted by the international ATA and EANM guidelines that only give recommendations for PET/CT imaging in the postoperative phase [1, 9]. This is also demonstrated by the results of our study; only 35 18F-FDG PET/CTs and 33 18F-DOPA PET/CTs were made preoperatively. In addition, more PET/CTs were performed in the UMCG than in the UMCU, highlighting the variability in decisions between hospitals, when no guidelines are available for guidance and when variability in tracer availability exists. In contrast, current guidelines do recommend routine performance of ultrasound in evaluation of thyroid nodules to guide risk stratification. It is therefore quite surprising that only 91 patients had a preoperatively ultrasound. In recent years, ultrasound use has likely become more standard compared to the earlier years of the study period. In addition, the retrospective nature may have caused an underestimation of the total preoperative ultrasounds.
While some groups advocate for extensive LND to improve nodal staging and reduce locoregional recurrences, others suggest a more conservative LND at primary treatment to reduce morbidity, while risking another operation later on. Impact of either approach on survival remains contradictory [3, 14,15,16,17]. The second approach was likely utilized by the tertiary referral hospitals in this study, as evidenced by the fact that 33% of patients underwent LND, confirming LNMs in a significant proportion of patients (90%).
In our study, 18F-FDG PET/CT and 18F-DOPA PET/CT performed particularly well in the detection of LNMs in the lateral compartment, with sensitivity rates of 89% and 81% and specificity rates of 100% and 100%, respectively. For 18F-DOPA PET/CT, the sensitivity is somewhat better while the specificity is concordant with literature (sensitivity 73–75%, specificity 100% [7, 18]). Comparable data for 18F-FDG PET/CT are unavailable. Conventional imaging modalities seem less sensitive and specific than either PET/CT. Interestingly, even ultrasound is slightly inferior to either PET/CT, according to our study. Limited data on the sensitivity and specificity of ultrasound for lateral LNMs in MTC varies between 58–89% and 71–97% [7, 19]. With PET/CT, a more targeted LND may be possible, optimizing the surgical strategy after diagnosis. Given that patients with lateral LNMs typically have simultaneous central LNMs, one could argue that identifying lateral LNMs is particularly critical as it establishes the need for both CND and LND. In this retrospective study, none of the imaging modalities gave a sufficiently high sensitivity and negative predictive value to safely rule out affected lateral neck lymph nodes and subsequent LND.
The standardized approach to perform a CND in MTC guidelines is reflected in our data. LNMs were identified in 51% of 140 patients undergoing a CND, which is comparable to literature [20, 21]. The sensitivity for LNMs in the central compartment was 72% on 18F-FDG PET/CT, but relatively low on 18F-DOPA PET/CT (39%). The latter is however in line with the only other reported sensitivity rates for central compartment LNMs in the preoperative setting (28% and 53%) [7, 18]. The discrepancy between 18F-FDG PET/CT and 18F-DOPA PET/CT is difficult to explain but may be the result of selection bias, where the observation of aggressive clinical course led to the choice for 18F-FDG PET/CT. However, in general, the low sensitivity for central LNMS on PET/CT imaging may be explained by simultaneous tracer uptake in the primary thyroid lesion, influencing visualization of small lymphadenopathy in the preoperative setting [22]. Ultrasound seems impractical for the assessment of central LNMs, likely because their anatomic position is further from the surface. Diagnostic CT may be best at localizing LNMs in the central neck, and could even be combined with PET. In the future, intraoperative fluorescent imaging may provide advanced information on affected lymph nodes to optimize the extent of the CND, on an individual basis [23].
Since total thyroidectomy remains the recommended treatment for patients with locoregional MTC, the role of PET/CT in identifying thyroid tumor bilaterality may appear insignificant. However, some studies suggest that hemithyroidectomy may suffice in patients with sporadic, unilateral disease when intraoperative frozen section assessment reveals absence of desmoplasia [24,25,26,27,28]. In this study, 18F-FDG and 18F-DOPA uptake was confirmed as true positive in 71% and 58% of cases, respectively. False-negative rates were relatively high as well, likely due to partial-volume effects and low tracer uptake in smaller tumors [7]. Moreover, in bilateral tumors confirmed by histopathology, imaging may have correctly identified only one tumor, leading to its classification as false negative. The false-negative rate for 18F-DOPA PET/CT was higher than for 18F-FDG PET/CT, likely due to a larger proportion of hereditary cases, in whom bilateral tumors are more prevalent. While PET/CT may reinforce the decision to perform a total thyroidectomy when bilateral uptake is detected, the high false negatives rates indicate that PET/CT alone is insufficient to justify de-escalating treatment to hemithyroidectomy.
Due to the unpredictable behavior of MTCs, determining the optimal surgical treatment for an individual patient can be challenging [29]. Current guidelines recommend routine ultrasound assessment of the thyroid and lymph nodes but this advice is mostly based on its performance in other thyroid cancers. Ultrasound is relatively inexpensive and safe, and cannot be replaced by PET/CT completely due to its value in obtaining fine needle aspiration cytology. However, for accurate evaluation, an experienced radiologist is required to obtain reliable information, and images are difficult to review later on. In contrast, PET/CT provides reproducible, whole-body images showing metabolic activity and basic anatomic information. While PET/CTs may be relatively expensive, the superior specificity and positive predictive value mean initial surgery can be optimized with the addition of an LND, lowering the risk of reoperating in a later phase. Moreover, the capacity of PET/CT to show distant metastatic disease can limit unnecessary surgery when cure is impaired anyways. The lower surgical (recurrence) costs and associated impact on the environment, may off-set the balance in favor of preoperative PET/CT imaging. Finally, relatively high 18F-FDG avidity may provide valuable information on tumor biology and support more aggressive management [10, 30,31,32]. As such, future guidelines should consider to implement advice on performing preoperative PET/CT imaging to optimize staging and treatment at diagnosis. While expensive, the findings may ultimately contribute to achieving cost reductions in the long run.
While this study included quite a large number of patients for such a rare disease, several limitations should be reported. Real-life retrospective data were used to evaluate our clinical practice patterns; as a result, not all patients underwent standardized PET/CT imaging and bilateral LND, restricting sensitivity and specificity calculations to those who were operated on, and probably inducing selection bias. Additionally, PET tracer uptake in lymph nodes was analyzed at the neck compartment level rather than by individual cervical levels, limiting precise correlations between tracer uptake and the histopathological presence of LNM. Nonetheless, we believe this approach enhanced the reliability of the data in this setting, as retrospectively pinpointing exact locations from nuclear physicians’ clinical reports is both challenging and prone to error. Finally, the actual images were not reviewed which means that reported values may be underestimated. Ideally, a future study should prospectively evaluate the influence of preoperative 18F-FDG PET/CT, and 18F-DOPA PET/CT on the surgical strategy, in a randomized, controlled study design and should incorporate preoperative biochemistry and assess the impact on cost-effectiveness and surgical outcomes.
In conclusion, PET/CT imaging can offer valuable insights to guide and personalize the initial surgical strategy, particularly when combined with a diagnostic CT. While PET/CT may optimize the necessity to perform a lateral neck dissection, diagnostic CT seems most optimal for staging of the central compartment. The additional capacity of PET/CT to provide information on the presence of distant metastatic disease means surgical management can be de-escalated when cure is improbable anyways.






Comments (0)