The boundaries between disease categories—between non-communicable (chronic) and communicable (infectious) diseases—are not as clear as they might appear at first glance. For instance, while HIV (human immunodeficiency virus) is a virus that attacks one’s immune system, infected people experience both acute infection and chronic disease that will transition into AIDS (acquired immune deficiency syndrome) without treatment (CDC 2022b). Likewise, COVID-19 may transition into long COVID, a chronic illness requiring care for an extended period (CDC 2024). Diabetes is not infectious in a traditional sense, yet narratives indicate the “spread” of diabetes across communities globally (Hu 2011; Rabin 2022). COVID-19 and diabetes were selected as representative conditions for their prominence in media discourses, for their prevalence globally, and for the urgency with which both conditions are characterized as pandemics in need of immediate action. Diabetes and COVID-19 also interact synergistically, leading to an increased number of deaths from both (Lv et al. 2022; Summan et al. 2024). Many individuals with COVID-19 infection who experienced hospitalizations and serious health complications had diabetes (Fang, Karakiulakis, and Roth 2020). It is important to acknowledge this link within and among disease categories in the discussion of healthcare priority setting as it makes distinguishing between and attributing effects of illness or death more complicated.
On January 30, 2020, the WHO Director General declared that the outbreak of COVID-19 constituted a Public Health Emergency of International Concern (WHO 2020). The significance and urgency of the COVID-19 pandemic was quickly recognized by the international community. The COVID-19 pandemic has tested national health crisis preparedness, supply chains, and manufacturing resilience. It resulted in significant economic setbacks and hampered travel and tourism globally. Unlike COVID-19, diabetes has a long history dating back to 1552 BC (Kilgour 1993). Diabetes impacts a patient’s ability to self-regulate blood glucose, which is vital for human life. T2D—over 95 percent of all diabetes cases—is considered a lifestyle disease and is a major cause of lower limb amputations, blindness, kidney failure, and cardiovascular disease. It also is a significant risk factor for adverse outcomes in infectious disease comorbidity. Both conditions have detrimental impacts on U.S. and global economies and mortality rates, yet they are approached very differently in terms of national and international efforts.
Risk Considerations
While COVID-19 is a novel virus, the discussions of an emerging new pathogen are not novel. National public health experts and the global health community had discussed the emergence of new pathogens, as well as national and global preparedness, for many years before COVID-19 made its appearance (Holloway et al. 2014). At the very core, these discussions are risk-based and aimed at easing the burdens of disease to human life and society. Emerging new pathogens or mutating known infectious agents create fear and speculation about the severity of the disease to come. Infectious diseases with pandemic potential are, therefore, an ongoing concern requiring proactive action to secure the best possible future with reduced risks to people and nation-states.
COVID-19 has real and perceived risks that are continually debated across all political levels. The real risks include the impact of disease on human health. They include the symptoms, health complications, hospitalization, and cost of testing and treatment. Additional risks include one’s inability to work and care for self and others, as well as the associated stress, anxiety, depression, and other mental health issues. They also include the impact of disease on one’s travel plans, one’s access to indoor and outdoor spaces, and one’s ability to infect others. The perceived risks are more challenging to define because they are future focused. They include the fear of the unknown, the uncertainty of the future impact of disease, possible mutations of the virus, and the long-term impact of the novel virus on one’s health, one’s well-being, and longevity. Additionally, perceived risks include the uncertain impact of infectious disease on the economy, society, and the government. The uncertainty prompts proactive steps and might be influenced by misunderstanding of real risks, by misinformation, or simply by the lack of knowledge.
Diabetes has a long history with rising rates of disease (CDC 2021b) and prediabetes (a condition of elevated risk factors for diabetes) in the United States (Sharpe 2020) with particularly worrisome trends among adolescents and young adults (Andes et al. 2020). Diabetes also has real and perceived risks. The real risks for diabetes include those highlighted for COVID-19 above, with some additional ones. These include the prolonged course of illness and lifelong disease management with associated high annual costs. Diabetes requires constant diligence to prevent irreversible complications and continuously degrading health. It can cause both short and long-term inability to work, chronic pain, discomfort, suffering, and life-long disability. Additionally, individuals with diabetes suffer from a wide range of psychiatric disorders, sleep disorders, eating disorders, and stress-related disorders at a higher prevalence than the general population (Brantly 2023). Diabetes also increases the risk of heart attack, stroke, foot ulcers, infection, limb amputation, blindness, and kidney failure (WHO 2023a) and elevates the risk of adverse effects from communicable diseases. There are fewer perceived risks for diabetes compared to COVID-19. These include genetic markers, family history of diabetes, ethnicity, and socioeconomic status that might necessitate frequent testing and the use of preventative pharmaceuticals. Perceived risks of diabetes are focused on the past, not the future. One’s ethnicity, family history, or genetic makeup cannot be changed over time. Perceived risks of diabetes also depend on the individual’s lifestyle and daily habits. While lifestyle and daily habits can change, it is up to the individual to change them. As a result, additional perceived risks of diabetes include individuals themselves, their behaviours, shortcomings, and their inability or unwillingness to follow prescribed regimens to achieve better health outcomes.
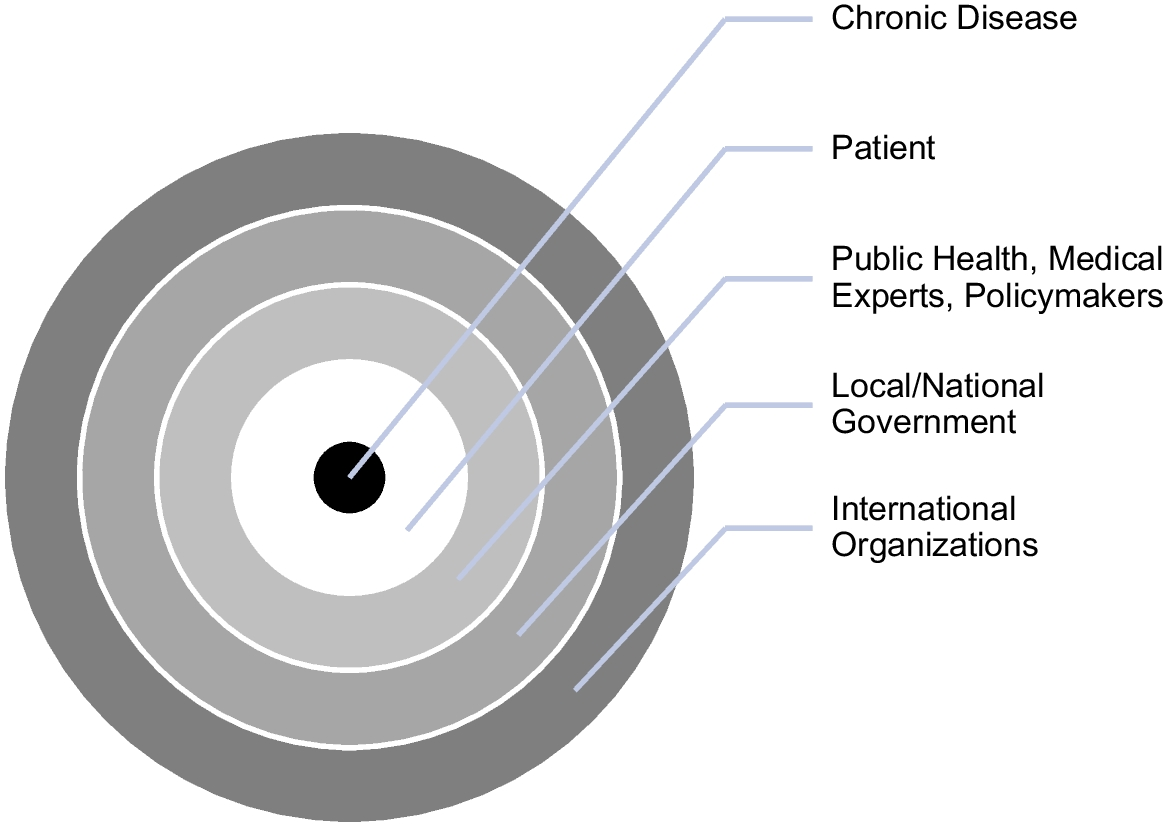
Both conditions have real risks that contribute to increased healthcare costs and suffering. Perceived risks for COVID-19 are future-focused. They seem to emerge from the outside of the body, from the infectious agent found in the environment. Diabetes perceived risks are focused on the past. Despite established social and environmental causes, perceived risks of diabetes seem to emerge from the inside of the body, from the genes or one’s poor choices. As a result, COVID-19 is perceived as a threat from the outside, necessitating a shared response to a common adversary. Diabetes, with a threat emerging within the individual, calls for personal responsibility and individual response. While COVID-19 appears to be non-discriminatory in how it affects others, everyone is at risk and in need of outside interference. Diabetes appears to affect individuals based on their choices or circumstances, so it requires vigilance and control from the self. Neither COVID-19 nor diabetes are social equalizers— quite the opposite; both expose how contemporary society depends structurally on the continuous production of differential vulnerability and varying levels of social disparities. However, perceptions about the risk and origin and expectations about these diseases might explain why approaches to address them differ so greatly.
Public Health Interventions
Early interventions for COVID-19 included nonpharmaceutical interventions such as personal hygiene, isolation, quarantine, and personal protective equipment (PPE) use. These measures have been studied extensively and shown to be effective in the prevention of communicable disease transmission (Peak et al. 2017). COVID-19–related lockdowns, while effective at halting the rapid spread of disease, adversely affected the provision of outpatient services, early diagnosis, and preventive treatments for a full range of health conditions. As a result of the lockdowns and physical distancing requirements, the utilization of telehealth services has increased. Public health efforts during the pandemic were helpful in curtailing the spread of the virus, facilitating access to care, and advocating for increased innovation and cooperation to ensure public health security.
International efforts in testing and vaccination development have resulted in record-breaking outcomes. The COVID-19 vaccine, an effective way to prevent severe infection (CDC 2023b), had to be prioritized by healthcare providers and at-risk population groups before nations had enough for their populations. However, existing fears and anxiety regarding vaccine acceptance and hesitancy were further impacted by the misinformation, lowering the intent to accept a vaccine and threatening the goal of achieving herd immunity against COVID-19 (Loomba et al. 2021). Additionally, the COVID-19 pandemic has redirected public health efforts and resources from other relevant issues, as well as increased the use of digital technologies to increase population surveillance, case identification, and tracking in the name of improved preparedness (Budd et al. 2020). Current efforts to address COVID-19 include vaccinations, home self-testing, and quarantine. These are reactive efforts. Proactive approaches include education, the stockpiling of vaccines, PPE, and biomedical equipment. They also include efforts to enhance preparedness for future infectious disease outbreaks, such as incentivizing domestic manufacturing to expand the supply chain related to future pandemics (FEMA 2020).
In 2010, the National Diabetes Prevention Program (NDPP) was created to address the increasing burden of T2D and prediabetes in the United States (CDC 2022c). The NDPP is a public-private partnership of many organizations focused on lifestyle change programmes to address diet and exercise to reduce the risks associated with T2D (CDC 2022c). However, such lifestyle-change programmes are usually short-term (up to a year) and offered at a cost; some are offered online only, and none address the underlying societal issues that contribute to the increasing prevalence of diabetes and prediabetes globally (CDC 2023d). The CDC, the American Diabetes Association (ADA), public health departments, and a variety of organizations are working on educational efforts, awareness campaigns, and interventions to inform the population of prediabetes and the risks associated with diabetes, targeting populations from adolescents to the elderly. Despite the resources currently available for diabetes education and prevention, there is still inequitable access to resources and issues with affordability.
Most public health efforts targeting diabetes are reactive and involve already-diagnosed individuals or those with prediabetes. Reactive approaches utilize data and biomedical technologies to manage disease using pharmaceuticals. Proactive efforts are very limited and primarily include education. In the United States, there are currently no population-level public-policy interventions aimed at creating improved conditions for all individuals through increased taxation, a ban on fast-food sales, or urban re-planning that necessitates physical movement of people. This tracks with scholarship arguing that there is a preference to maintain the disease-promoting lifestyle by ingestion of pharmaceuticals over taking action to impose restrictions to effect change (Greene 2007). Some limited approaches have been adopted in countries such as Brazil, India, Ireland, the United Kingdom, and South Africa, which have focused on the taxation of sugar-sweetened beverages (Kruger et al. 2021). Diabetes can be characterized as a social problem, indicating the need to focus on population-level mitigation and prevention efforts. However, a contrary characterization is more often applied, with the emphasis placed on individual responsibility in diabetes discourses that are closely tied to obesity discourses (Guthman 2009).
Interestingly, diabetes discourses themselves can induce stress, anxiety, and mental health issues, impeding efforts to educate and encourage action of self-control and lifestyle change. Despite these challenges, individuals diagnosed with diabetes are often viewed as offenders since they do not follow established norms and expectations of self-care. Thus, public health approaches to diabetes are likely to focus on education and self-management. Individuals diagnosed or at risk of COVID-19 are often viewed as victims of an external environmental threat. Thus, approaches to COVID-19 require collective action and focus on greater public health interventions. COVID-19 is perceived as a collective enemy, similar to the invasion of a political adversary. It is a virus that calls for common responsibility and necessitates a joint response. As a result, no fault is ascribed to people who fall ill due to COVID-19, as the fault rests with the viral threat. Diabetes, by contrast, involves no such apparent invasion and is therefore considered to emerge from an innate flaw in the individuals themselves. In fact, those with diabetes are seen as a threat to the state because of their perceived irresponsibility, cost to the public, and fragile biological constitutions.
Funding Priorities
With the emergence of COVID-19, the fear, hype, and significance of the emerging pathogen redirected the attention and funding of individuals, businesses, and governments towards a single adversary that endangered human health. The Centers for Disease Control and Prevention (CDC) was awarded a total of US$2 billion from the American Rescue Plan to bolster the governmental public health response to the COVID-19 pandemic and to establish, expand, and sustain a public health workforce (CDC 2021c). This is a significant increase in funding to support the hiring of personnel at the local health department or community-based organization level dedicated to COVID-19 efforts. In 2020, the CDC was awarded nearly $730 million in funding intended “to carry out surveillance, epidemiology, laboratory capacity, infection control, mitigation, communications, and other preparedness and response activities” (CDC 2023a). The funding received by the CDC for COVID-19 assistance and relief as of August 2021 amounted to over US$67 billion (CDC 2021a). USAspending.gov, which tracks federal awards, loans, and federal assistance, reported total COVID-19 spending in the amount of US$3.6 trillion across different U.S. agencies (2023).
The WHO worked on a global scale to “combat the COVID-19 pandemic” through the Strategic Preparedness and Response Plan (WHO 2021). Despite some funding gaps (WHO 2022), governments around the world took extensive action to reduce and limit the economic and human impact of the COVID-19 pandemic (IMF 2022). The pandemic was able to generate not only significant financial resources but also the unified action of a diverse group of stakeholders. Expenditures related to COVID-19 might be perceived as investments into risk-reduction efforts and improved future pandemic preparedness. This investment is expected to bring forth worthwhile results in the form of vaccines and other pharmaceuticals and biomedical technologies, as well as greater security, improved productivity, and less risk. Approaches to COVID-19 appear to spur commercial production that supports corporate profitability.
Diabetes is a costly condition for both individuals and healthcare systems. In addition to the high and continuously increasing costs of diabetes care in the United States (Riddle and Herman 2018) and the loss of productivity, individuals living with diabetes rely on affordable healthcare services and treatments, including insulin, for their survival (PAHO 2022). In September 2018, the CDC awarded US$45 million to state health departments of all fifty states and the District of Columbia under a new five-year cooperative agreement for T2D prevention and management efforts (CDC 2021d). Despite these efforts, many U.S. residents are living with a chronic condition, with nearly 50 per cent of individuals over the age of fifty-five having two or more chronic conditions (RFAH 2021). Additionally, diabetes is one of the largest global public health concerns, with negative effects on public health and socio-economic development around the world (Lin et al. 2020). It carried with it significant costs in terms of mortality and reduced life expectancy. The global costs of diabetes are also increasing, with the global economic burden of diabetes expected to increase from US$1.3 trillion in 2015 to US$2.5 trillion by 2030 (Bommer et al. 2018).
COVID-19 is associated with an acute onset of disease and a rapid impact on society with a high level of threat to national and global economies. Diabetes is associated with slow onset, slow impact on society, and a lower level of immediate threat to the economy. Chronic disease appears to be perceived as a choice driven by one’s ignorance towards societal standards set for a healthy lifestyle, including daily exercise (CDC 2022a) and healthy food consumption (USDA 2024). This ignorance is then coupled with the determination of deservingness. Diabetes is determined to be unworthy and undeserving of increased funding and other public resources because it might be considered malleable, flexible, and fixable with changes in one’s lifestyle, with increased awareness and education. On the other side, infectious disease is perceived as a fixed category beyond one’s control, requiring collective response via vaccination, travel restrictions, and work-from-home policies.
Despite the estimates that every dollar invested in proven non-communicable disease interventions in low- and lower-middle-income countries will generate at least seven dollars in “increased economic development or reduced health care costs by 2030” (CDC 2021e), expenditure related to diabetes are less likely to be viewed as a good investment. Proactive approaches to diabetes can be seen as long-term investments without short-term returns. It means giving up resources today for a potential chance to improve health in the future. Long-term investments are risky as they do not offer an immediate return on investment. It is easier to shift the responsibility to the individual to make better choices in the system designed to motivate them to do otherwise than to change the system itself. These calculations, in turn, shape the biopolitical decisions that determine whose lives are worth investing in and who, by contrast, should be starved of resources.
Both conditions are closely tied to commercial interests and commercial activities. While the focus on COVID-19 is aimed primarily at treatment and preparedness, the focus with diabetes is on disease management and education. The big business of diabetes management and the growing market of pharmaceuticals is chronologically related to specific screening, diagnosis, treatment, and diabetes management guidelines modifications (Hunt et al. 2021). It is more cost-effective to manage diabetes than to prevent or cure it. As a result, health becomes a form of human capital to be invested in, researched, and developed (Kenny 2015). It becomes a matter of commercial, scientific, and political reasoning and manipulation. Health becomes an economic project with pros and cons for investment, with returns and losses, as well as short- and long-term considerations.




Comments (0)