In recent years, imbalance between gastrointestinal peptides such as acyl-ghrelin, motilin and NPY, and anorectic peptides such as pro-opiomelanocortin has been implicated as a cause of CINV and anorexia in cancer patients [11]. To date, only a few reports have examined the relationship between gastrointestinal peptides and CINV or post-chemotherapy anorexia, focusing on a single peptide or a few peptides [20, 21]. The present study comprehensively evaluated the changes in blood levels of plasma gastrointestinal peptides and the association with CINV and anorexia. The new findings are as follows: (1) plasma NPY and leptin were elevated and plasma acyl-ghrelin tended to decrease in the early phase of the chemotherapy session; (2) plasma motilin increased significantly on days 5 and 8 compared to baseline only in the CINV group, and the levels were significantly higher in the CINV group than in the non-CINV group; (3) plasma leptin remained significantly higher on day 5 compared to baseline only in the anorexia group.
Platinum-based drugs such as cisplatin cause many adverse events via 5-HT, such as renal damage, bone marrow suppression and digestive dysfunction. Cisplatin dose-dependently reduces plasma ghrelin level in rats, and the response is mediated by 5-HT3 or 5-HT4 receptors [22]. In our study, all patients received a 5-HT3 receptor antagonist (palonosetron) only for the first 24 h. Ten patients did not fulfill the definition of anorexia, but reduced appetite and decreased plasma ghrelin levels were observed from day 3 of the chemotherapy session, suggesting that the 5-HT3 receptor antagonist may be ineffective in preventing anorexia. Substance P and NK1 receptors are associated with late-onset CINV. Aprepitant inhibits the binding of substance P to the NK1 receptor in the vomiting center, and is effective for late-onset CINV that cannot be prevented by 5-HT3 receptor antagonists and manifests within 120 h after cancer chemotherapy [3, 4]. In this study, all patients received fosaprepitant prior to chemotherapy, but plasma substance P levels on days 3 and 5 did not increase compared to baseline. In addition, no significant differences in plasma substance P levels were observed between the CINV and non-CINV groups throughout the observation period. These findings suggest that CINV occurring in this study may be due to mechanisms other than the substance P–NK receptor pathway.
Plasma motilin levels increased significantly compared to baseline in the relatively late phase of the chemotherapy session only in the CINV group, and the levels were significantly higher in the CINV group than in the non-CINV group. Motilin is a hormone secreted by the upper gastrointestinal tract during fasting and is responsible for controlling the interdigestive MMC [23]. This hormone stimulates gastrointestinal peristalsis and promotes digestion, but excessive secretion enhances the interdigestive MMC causing nausea [24]. Therefore, the cause of CINV is speculated to be excessive secretion of motilin due to chemotherapy-induced loss of appetite.
Plasma acyl-ghrelin levels decreased following chemotherapy in 15 of 18 patients. Ghrelin has a variety of physiological activities and therefore has attracted attention in various fields. In particular, the effect of ghrelin in increasing food intake is well known, and the mechanism of action has been elucidated. Ghrelin is secreted by the stomach during fasting and stimulates food intake. In addition, signals are transmitted from the periphery to the brain via humoral or nervous pathways to suppress energy expenditure and maintain energy balance [25, 26]. Ghrelin affects the digestive system, stimulating gastric acid secretion and gastric emptying. Plasma acyl-ghrelin level increases before meal, peaks at the beginning of a meal, and returns to basal level within one hour after meal. Hiura et al. [20]. demonstrated that plasma total ghrelin levels decreased significantly on days 3 and 8 of cisplatin-based chemotherapy and were associated with cisplatin-induced anorexia. Rikkunshi-to, a traditional herbal medicine, increases plasma ghrelin level in rats and is effective against cisplatin-induced anorexia [22]. In a previous preliminary experimental study, electro-acupuncture was effective for chemotherapy-induced anorexia by upregulating plasma ghrelin level [27]. These effects may be associated with increased secretion of appetite-related peptides including ghrelin and NPY. However, in this study, no significant difference in plasma acyl-ghrelin level was observed between the anorexia and non-anorexia groups throughout the observation period.
Plasma level of leptin, an appetite-suppressing hormone, was significantly elevated on day 3, regardless of anorexia. However, the level remained significantly higher on day 5 compared to baseline in the anorexia group, whereas the level decreased and was not significantly different from baseline in the non-anorexia group. This finding suggests that anorexia may be related to the prolonged increase in leptin secretion in the late phase of the chemotherapy session. Leptin and ghrelin have opposite physiological functions in energy homeostasis: leptin inhibits food intake while ghrelin stimulates appetite [28]. Consistent with these characteristics, leptin and ghrelin levels fluctuated in opposite directions during the chemotherapy session. However, leptin does not regulate ghrelin secretion, and both peptides function independently in controlling energy homeostasis [28]. This may partially explain why, in contrast to leptin, no significant differences in acyl-ghrelin level were observed between the anorexia and non-anorexia groups.
The results of this study indicate that regulation of the substance P‒NK1 receptor pathway alone is not sufficient to suppress late-onset CINV. The present results also suggest that excessive motilin secretion may be responsible for the occurrence of nausea. Motilin is a peptide hormone that is secreted during fasting, and if anorexia occurs after chemotherapy, motilin secretion would be excessive and cause nausea. Two of the four patients who actually developed CINV had anorexia, and the other two had anorexia from baseline. Therefore, it is important to improve anorexia in order to control nausea, which may be achieved by using dopamine D2 receptor blockers such as metoclopramide and domperidone, or Rikkunshi-To.
Differences in patient-specific factors such as baseline nutritional status may also influence peptide secretion dynamics and the development of anorexia. The present data show a tendency of lower serum albumin levels in the anorexia group compared to the non-anorexia group (3.4 g/dL vs. 3.9 g/dL, p = 0.06). Previous reports have shown a negative correlation between albumin and leptin levels in the elderly and patients on dialysis [29, 30]. Taken together, these findings suggest that baseline nutritional status may contribute to the prolonged increase in leptin concentration observed in the anorexia group. In addition, although there are no reports of a correlation between albumin and motilin concentrations, when anorexia is accompanied by hunger, motilin is overproduced, which also leads to nausea. On the other hand, albumin level correlates inversely with leptin level, suggesting increased leptin secretion in a hypoalbuminemic state, causing anorexia. Thus, patients with low albumin levels may be more susceptible to develop anorexia and nausea.
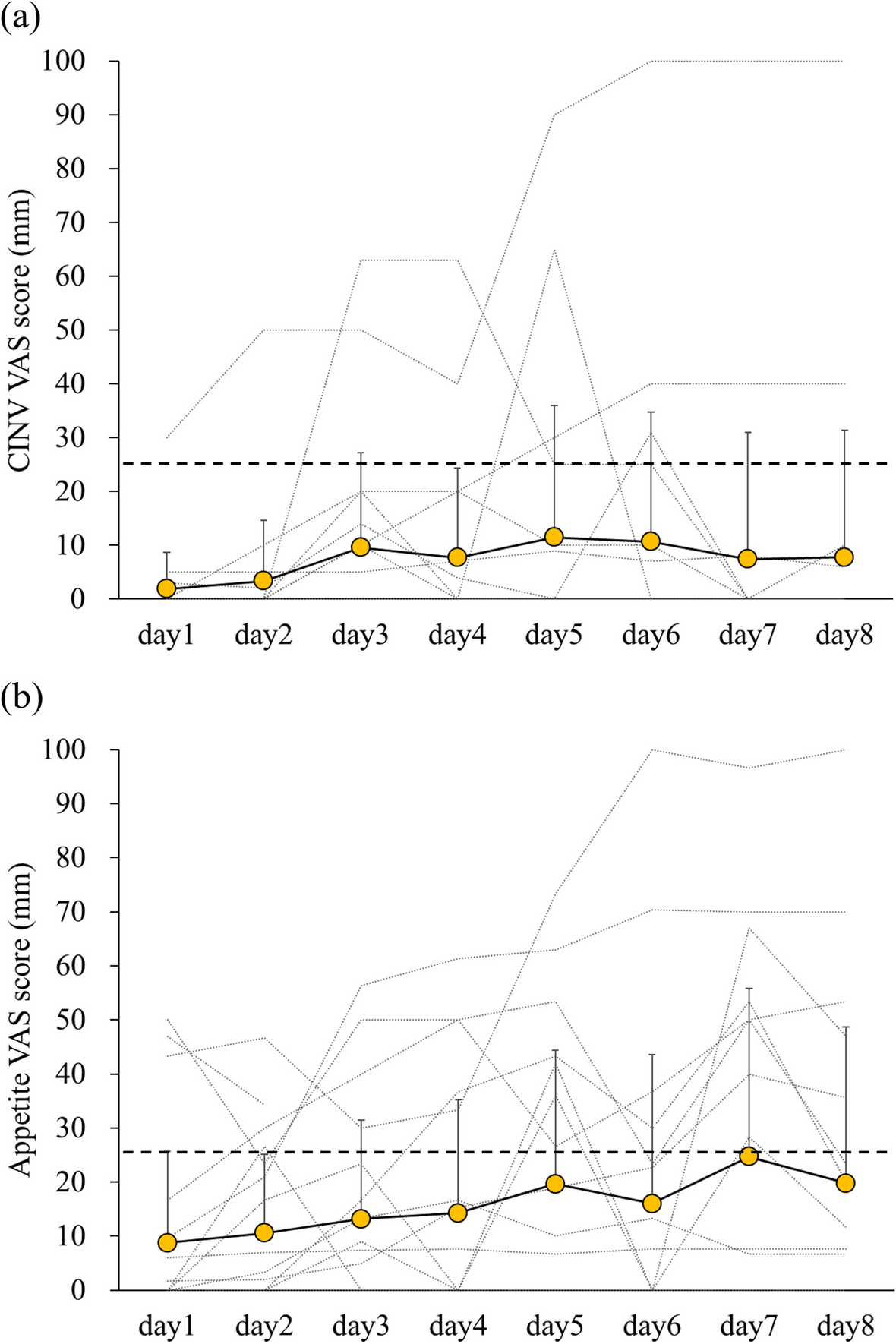
This study had several limitations. First, in this single-center prospective cohort study in patients with esophageal cancer and urothelial cancer or testiculoma treated with a cisplatin-based regimen, only 20 patients were recruited during the study period. The small sample size may have resulted in insufficient statistical power to detect significant differences in plasma levels of peptides other than motilin and leptin between CINV and non-CINV groups, and between anorexia and non-anorexia groups. The small sample size was a key limitation of this study, which may have reduced the credibility of the results. While the detected effect sizes for the statistical tests were relatively high (Table S1), a large-scale multicenter study is needed to verify the present findings in the future. Second, we employed the VAS scale to score the severity of nausea and anorexia. The VAS scale was originally developed by Keel [31] as a simple descriptive pain scale. The VAS questionnaire has been modified to assess appetite, and the reproducibility and validity have been demonstrated [32, 33]. However, since this method depends on the subjective rating of the patient, it is undeniable that the score may be affected by the patients’ background when the number of samples is small. To address this problem, a large-scale study would also be necessary in the future. Third, the timing of cisplatin administration differs among chemotherapy regimens (CDDP/5-FU, day 1; CDDP + GEM, day 2; CDDP + BLM + ETP, days 1–5), which may influence the dynamics of gastrointestinal peptides, as well as the development of CINV and anorexia. However, a subanalysis of the effect of different chemotherapy regimens on the changes in plasma levels of the five peptides indicated minimal impact of CDDP schedule on the changes in peptide levels, with the exception of NPY (Figures S1-S5). Although CDDP + BLM + ETP includes five days of CDDP infusion, motilin levels remained almost stable during chemotherapy session, resulting in no patients developing CINV. Furthermore, although CDDP given on day 2 of GEM + CDDP therapy may conceivably shift the peak of motilin levels, no marked difference was observed visually between CDDP/5-FU and GEM + CDDP. Given the small number of patients who received GEM + CDDP or CDDP + BLM + ETP therapy and developed CINV or anorexia, further study is warranted to evaluate the impact of different chemotherapy regimens. Fourth, the number of chemotherapy cycles differed between patients. This variation may influence the development of CINV or anorexia, as these adverse events are more likely to occur during the first treatment cycle. However, no differences in changes in peptide levels between the first chemotherapy cycle and subsequent cycles were observed by visual assessment (Figure S6), suggesting minimal impact of chemotherapy cycle on the dynamics of gastrointestinal peptides. Since the number of study patients was limited, further study is warranted to evaluate the influence of chemotherapy cycle.





Comments (0)