
Remember me
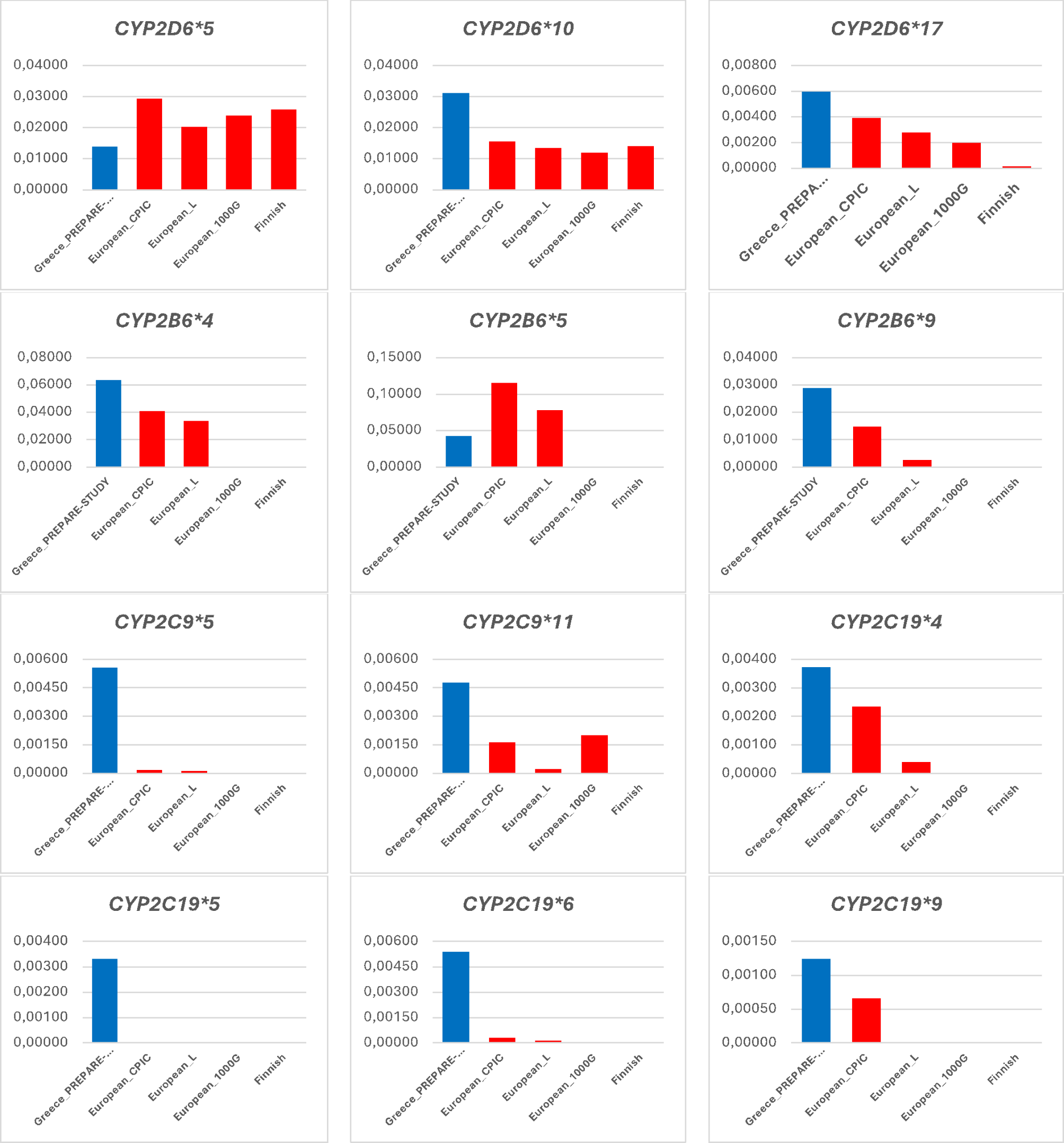



Our genotyping approach has demonstrated differences in the prevalence of 17 PGx biomarkers in seven pharmacogenes between the Greek population and the European average, deducted from more than one source as summarized in Figs. 1 and 2. In particular, there are four PGx biomarkers in the CYP2C19 gene, namely CYP2C19*4, CYP2C19*5, CYP2C19*6 and CYP2C19*9, two PGx biomarkers in the CYP2C9 gene, namely CYP2C9*5 and CYP2C9*11, two PGx biomarkers in the CYP2B6 gene, namely CYP2B6*4 and CYP2B6*9, two PGx biomarkers in the CYPD6 gene, namely CYPD6*10 and CYPD6*17, and one PGx biomarker in each one of the SLCO1B1 and TPMT genes, namely SLCO1B1*5 and TPMT*3 C, respectively, that present with higher allelic frequencies (more than 2-fold) compared to the European average from at least two of the available sources. Also, there are two PGx biomarkers in the TPMT gene, namely TPMT *3A and TPMT *3B, and one PGx biomarker in the CYP2D6, CYP2B6, and DPYD genes, namely CYP2D6*5, CYP2B6*5, and DPYD:c.2846 A > T, respectively, that present with lower allelic frequencies (more than 2-fold) compared to the European average from at least two of the available sources. Data from the Finnish population and the 1000G project were not available for a few pharmacogenes such as TPMT, SLCO1B1 so there were not represented in Figs. 1 and 2. In those cases, comparisons were made based on CPIC data or available literature for the European population.
Fig. 1
Prevalence of PGx biomarkers in the pharmacogenes in the CYP450 family in the Greek population (in blue), compared to the European average, as documented in the CPIC database, the 1000 Genomes project, the literature, and the Finnish population (in red). Abbreviations: European_L: European population data extracted from the literature, European_1000G: European population data extracted from the 1000 Genome project, European_CPIC: European population data extracted from the Clinical PGx Implementation Consortium
Fig. 2
Prevalence of PGx biomarkers in other pharmacogenes in the Greek population (in blue), compared to the European average, as documented in the CPIC database, the 1000 Genomes project, the literature, and the Finnish population (in red). Abbreviations: European_L: European population data extracted from the literature, European_1000G: European population data extracted from the 1000 Genome project, European_CPIC: European population data extracted from the Clinical PGx Implementation Consortium
We have also calculated the prevalence of the different metabolizer statuses in the different pharmacogenes analyzed herein (Table 1; Fig. 3). At the gene level, VKORC1 (74.94%), UGT1A1 (52.53%) and CYP2D6 (43.81%) were the top genes with the highest frequency of actionable phenotypes, reflecting on warfarin (VKORC1), atazanavir, irinotecan (UGT1A1) and most importantly a variety of medications, such as psychiatric, antihypertensive, antiarrhythmic, tamoxifen, codeine, tramadol and others (CYP2D6). CYP3A5, TPMT, and DPYD had the lowest frequencies of actionable phenotypes, namely 0.07%, 4.7%, and 4.9% respectively, in line with the expected population prevalence and confirming findings from our previous pilot study [7].
Table 1 Frequencies of the various metabolizer statuses in the different pharmacogenes analyzed for the purpose of this study (see also Fig. 3)Fig. 3
Frequencies of the various metabolizer statuses in the different pharmacogenes
Academic PGx research laboratories and faculty membersTwo academic research laboratories bear PGx in their official title. The Laboratory of Pharmacogenomics and Individualized Therapy of the University of Patras, department of Pharmacy (www.permed.upatras.gr) is involved in PGx research using a holistic approach, namely from the wet- and dry-lab and public health genomics perspectives [17]. This laboratory was also involved in the PREemptive Pharmacogenomic Testing for Preventing Adverse Drug Reactions (PREPARE) clinical study (see below). Also, the Laboratory of Molecular Genetics and Pharmacogenomics/Toxicogenomics of the department of Molecular Biology and Genetics, Democritus University of Thrace (DUTH) is involved in PGx research, although none of its faculty members bear PGx in their official academic titles. In addition, the Clinical Genomics and Pharmacogenomics Unit belongs to the 4th Pathology Clinic of the School of Medicine of the National and Kapodistrian University of Athens (NKUA), whose members are also involved in PGx research. There are also a few other academic laboratories that are involved in PGx research activities, but they do not bear PGx as a term in their official titles.
There are four faculty members in Greece that bear PGx in their official academic title and are involved in PGx research; one at the DUTH, Faculty of Medicine, Laboratory of Pharmacology, one at the School of Medicine Clinical Genomics and Pharmacogenomics Unit at NKUA, one at the Aristotle University of Thessaloniki, department of Pharmacy, Thessaloniki and the author’s Institution, namely the University of Patras, department of Pharmacy, Laboratory of Pharmacogenomics and Individualized Therapy, Patras. The author was also a Full member and National Representative of Greece at the European Medicines Agency, CHMP-Pharmacogenomics Working Party from July 2010 until December 2022, at which time the Working Party was retired by the EMA and integrated into the Methodology Working Party.
PGx education at the undergraduate and postgraduate level in GreeceOur findings from a web-based survey that was conducted in May 2024 have revealed some differences compared to our previous analysis performed in March 2014 [16] as far as PGx education in Greece is concerned.
At the undergraduate level, we have assessed the latest curricula of the Schools/Faculties/Departments of Medicine, Pharmacy, and Biology of all Greek Universities. Of the seven Medical Faculties in Greece, the Faculty of Medicine of the University of Ioannina (UoI) and the one of DUTH have an elective course dedicated to PGx, while all other five Medical Faculties/Schools have sessions dedicated to PGx, as part of other compulsory or elective courses on Pharmacology. From the three departments of Pharmacy, the University of Patras (UPAT) has an compulsory course dedicated to PGx, the Aristotle University of Thessaloniki (AUTH) has an elective course dedicated to PGx, while there is no such dedicated PGx course at the department of NKUAbut only discusses PGx topics as part of the Pharmacology course. Based on our research, there is no compulsory or elective course focused on PGx at the four biology departments of Greek Universities. However, the PGx topic is included in the undergraduate curricula, as part of courses on Human Genetics, Human Molecular Genetics, Genomics, Biochemical Pharmacology, and Clinical and Pharmaceutical Biotechnology in three departments out of the four. More precisely, Molecular Biology and Genetics (DUTH), Biochemistry and Biotechnology (University of Thessaly; UTH), and Biotechnology (Agricultural University of Athens) have a dedicated PGx course. On the contrary, the department of Biology of the University of Crete (UoC) has no course or session dedicated to PGx.
At the postgraduate level, PGx stand-alone courses and lectures in related courses are available both in departmental and interdepartmental and inter-institutional graduate programs. In the first case, among eight Universities in Greece, only the UPAT and the UTH provides stand-alone PGx courses, while four Universities (in Patras, Athens, Thessaloniki and Thessaly) include PGx topics in related courses in five of their graduate programs (Fig. 4A). As far as interdepartmental and inter-institutional graduate programs are concerned, the UPAT and DUTH provide stand-alone PGx courses in their interdepartmental graduate programs on Personalized Medicine, while four Universities in Patras, Athens, Thessaloniki and Thrace discuss PGx topics in related courses in 5 of their interdepartmental and inter-institutional graduate programs (Fig. 4B). The University of Crete does not have any stand-alone PGx course or PGx lecture in its three related graduate programs.
Fig. 4
Overview of the departmental (A) and interdepartmental/interinstitutional (B) postgraduate courses that have stand-alone PGx courses (in green) and/or discuss PGx topics within other related courses in Greek Universities (total number of courses in blue). UOC: University of Crete, UOI: University of Ioannina, DUTH: Democritus University of Thrace, UTH: University of Thessaly, AUTH: Aristotle University of Thessaloniki, NKUA: National and Kapodistrian University of Athens, UniWA: University of Western Attica, UPAT: University of Patras, Med: Department of Medicine, Pharm: Department of Pharmacy. Asterisk depicts universities with stand-alone PGx courses
Clinical implementation studies on genome-guided therapeuticsTwo multinational, multicenter, prospective PGx clinical implementation studies have been performed in Greece. The European Pharmacogenetics for AntiCoagulant Therapy project (EU-PACT; NCT01119300, https://clinicaltrials.gov/ct2/show/NCT01119300) included two single-blind, randomized trials that aimed to compare a genotype-guided dosing algorithm that included clinical variables and genotyping for CYP2C9 and VKORC1 with a dosing algorithm that included only clinical variables, for the initiation of warfarin, acenocoumarol or phenprocoumon treatment in patients with atrial fibrillation or venous thromboembolism [18, 19]. The primary outcome was the percentage of time in the target range for the international normalized ratio (INR; target range, 2.0 to 3.0) within a 12-week period after the initiation of therapy. In the clinical study, four countries were involved in patient recruitment, namely the UK (warfarin, acenocoumarol, phenprocoumon), Sweden (warfarin), Greece (acenocoumarol), and the Netherlands (acenocoumarol, phenprocoumon). In Greece, a total of 207 patients were recruited from three sites across Greece; the University General Hospital of Alexandroupolis, Democritus University of Thrace, Faculty of Medicine, and the Onassis Cardiac Surgery Center in Athens, Greece. The EU-PACT study concluded that PGx-guided dosing of warfarin was associated with a higher percentage of time in the therapeutic INR range compared to standard care during the initiation of warfarin therapy, whereas PGx-guided dosing of acenocoumarol or phenprocoumon didn’t show any relevant improvement during the 12 weeks after the initiation of therapy.
Moreover, a second study, namely the PREemptive Pharmacogenomic testing for Preventing Adverse Drug Reactions study (PREPARE; NCT03093818; https://classic.clinicaltrials.gov/ct2/show/NCT03093818) was an open-label, multicentre, controlled, cluster-randomized, crossover implementation study of a 12-gene pharmacogenetic panel in 18 hospitals, nine community health centers, and 28 community pharmacies across seven European countries (Austria, Greece, Italy, the Netherlands, Slovenia, Spain, and the UK) [13]. Having recruited a total of 6944 patients with primary indications spanning several medical specialties including oncology, cardiology, psychiatry, and so on, it was shown that genome-guided treatment using a 12-gene PGx panel significantly reduced the incidence of clinically relevant adverse drug reactions and was feasible across diverse European health-care system organisations and settings. In Greece, 1326 psychiatric patients were recruited in total at two sites; the University General Hospital of Patras and the ATTIKON University General Hospital in Athens, Greece [20].
Private and public PGx service providers in GreeceOur data show that there are nine out of 21 private genetic laboratories in Greece that offer PGx testing services (41%). Also, there is only one public (academic) PGx laboratory that offers PGx testing services that is also accredited for PGx services by the European Molecular Diagnostics Quality Network. Most of these offer PGx testing services for various medical specialties and/or medications, while some of them specialize in specific medical specialties such as oncology or psychiatry.
It seems that no new private or public laboratories have incorporated PGx services in their flow. According to our previous studies, the number of genetic laboratories that offer PGx testing services remains more or less unaltered (41% compared to 44% in 2011; 15), even though few of them have discontinued their operations, while others were founded. This observation does not give a clear picture of the actual demand for this type of services in the market. In other words, it is unclear whether there is a significant interest of healthcare professionals to prescribe such testing even though there are specialized laboratories who offer them. It must be noted that only a couple of PGx tests for oncology and, recently, for psychiatry are being reimbursed by the public payer. The latter test, however, also includes genomic variants that are not clinically actionable, which questions the clinical validity of this test, as the result provided to the patient/treating physician is not fully approved by the EMA or any other regulatory body worldwide.
Regulatory guidance for genome-guided drug dose adjustment in GreeceWe have previously revealed a vast discrepancy among the regulatory guidance for PGx-guided treatment among the different regulatory bodies worldwide [21, 22]. As such, this has prompted us to inquire whether such discrepancy also exists between the Greek NOM and its supervisory body, namely the EMA and the Galinos Greek medicines repository.
Interestingly though, there is a vast discrepancy between the medications that have PGx guidance for drug dose adjustment in the SmPCs as documented in the Greek NOM and Galinos, compared to the EMA. In particular, there are 140 active compounds available in the EMA drug annotations list, as shown in the PharmGKB database. From these, there are only 31 active compounds that are documented in the Greek NOM and the EMA (22.14%), while only 25 active compounds are listed in Galinos and the EMA (17.86%). Moreover, only four active compounds are documented in the Galinos and the Greek NOM (2.86%; Fig. 5). Evidently, there is a big difference between the number of active compounds listed in the Greek NOM and Galinos per se, and the indications that these medications refer to. In particular, 28 out of 31 active compounds in the Greek NOM refer to anticancer medications and three out of 31 refer to medications for diabetes, while the 25 active compounds listed in the Galinos resource were more diverse since they belong to five anticancer medications, four antiviral, three psychiatric medications, two medications for the urinary system and 11 for other indications. Three of four active compounds that are present both in the Greek NOM and the Galinos are anticancer medications, namely irinotecan (UGT1A1), capecitabine (DPYD), and erlotinib (EGFR), while one is an antidiabetic medication namely glibenclamide (G6PD). It is noteworthy that although the Greek NOM is a formal member of the EMA, only 22.14% of the medications with approved PGx information in their labels by the EMA are listed.
Fig. 5
VENN diagram indicating the vast discrepancy between the medications that have PGx guidance for drug dose adjustment in the SmPCs as documented in the Greek NOM and Galinos, compared to the EMA (see also text for details)
Comments (0)