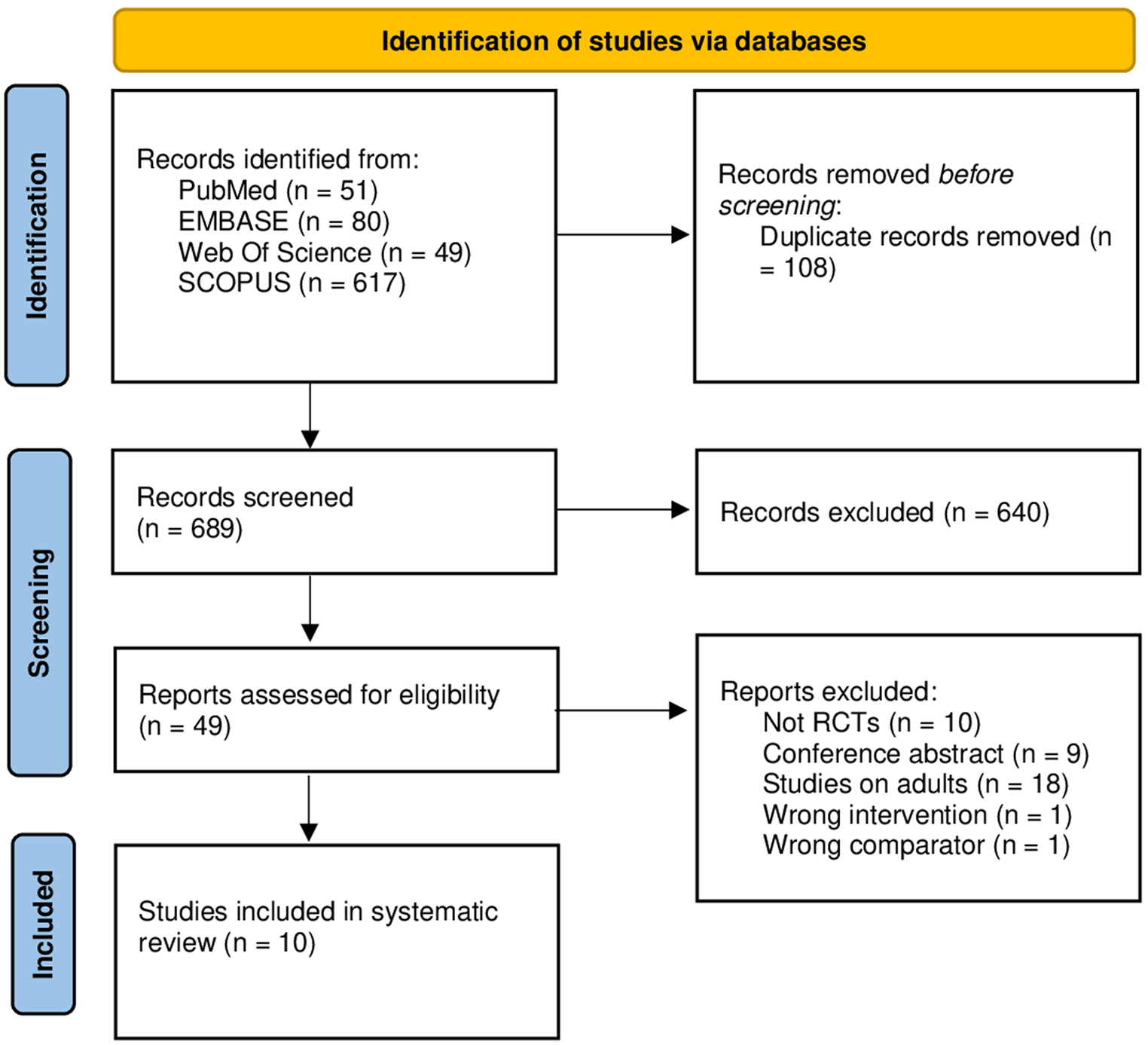
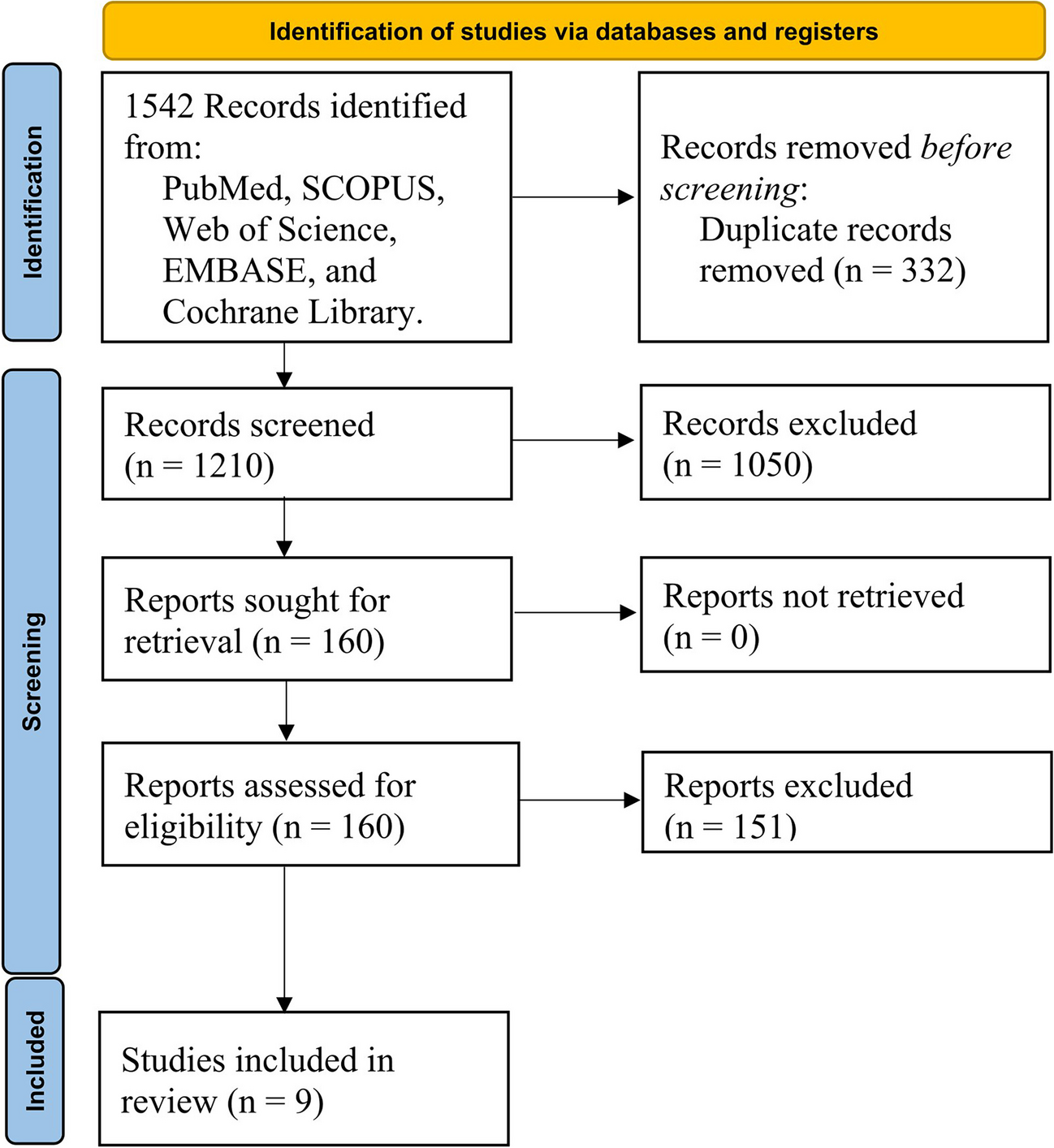
This systematic review and meta-analysis synthesized data from nine retrospective cohort studies involving 346 pediatric patients with pericarditis evaluated in emergency settings. The findings highlight the importance of recognizing pericarditis in pediatric patients, given its distinct clinical presentation and significant diagnostic markers. The high prevalence of chest pain (87.5%) reaffirms its significance as a primary symptom of pericarditis in pediatric patients presenting in emergency settings. Fever (71.3%) and dyspnea (26.3%) were also common, and their presence, along with chest pain, should prompt clinicians to consider pericarditis. This aligns with previous findings, which reported chest pain as the primary symptom in both adult and pediatric pericarditis, with children often exhibiting more systemic symptoms like fever and fatigue [6, 23]. Such recognition is crucial for timely diagnosis and management, which can significantly affect patient outcomes.
Electrocardiographic (ECG) changes are pivotal in diagnosing pericarditis. ST-segment elevation was observed in 63.8% of cases, underscoring its diagnostic importance. However, the presence of normal ECGs in 27.0% of patients suggests that pericarditis can present with varied ECG findings, necessitating a thorough clinical evaluation [24]. This variability in presentation emphasizes the need for a comprehensive diagnostic approach, including ECG and imaging studies [3]. Imaging findings further aid in diagnosis and management. Normal chest radiographs were seen in 60.3% of cases, while cardiomegaly was noted in 86.6%. Echocardiography revealed pericardial effusion in 80.1% of patients and cardiac tamponade in 12.9%. These findings align with previous reports, highlighting the variability in radiographic presentations of pericarditis [22].
It is worth noting that the heterogeneity observed across clinical practices, including differences in diagnostic tools such as ECG interpretation, suggests the need for standardized protocols. This variability may stem from differences in regional clinical practices, study design, or sample sizes.
Such imaging studies are essential for identifying complications and guiding treatment. The consistent elevation of C-reactive protein (CRP) levels (mean 12.042 mg/dL) reflects the inflammatory nature of pericarditis and supports its diagnosis. Elevated CRP levels help differentiate pericarditis from other causes of chest pain and guide the intensity and duration of anti-inflammatory treatment [25]. This observation is consistent with reports that noted elevated inflammatory markers as common in pediatric pericarditis [25]. Monitoring CRP levels can provide valuable insights into the patient’s response to therapy and disease progression.
High admission rates (88.6%) indicate the severity of pediatric pericarditis and the necessity for inpatient care to monitor and manage potential complications. Despite the condition’s severity, the low mortality rate (6.8%) suggests a favorable prognosis with timely and appropriate medical intervention. These findings underscore the effectiveness of current treatment protocols, including the use of anti-inflammatory medications and careful monitoring for complications [13]. Early recognition and intervention are critical in improving patient outcomes and reducing mortality.
Standardized protocols for ECG interpretation, imaging studies, and inflammatory marker assessment can help mitigate the observed variability in diagnostic practices and improve patient care.
When comparing these findings to previous studies, it is evident that the clinical presentation of pediatric pericarditis shares similarities with adult presentations, particularly in terms of chest pain and fever being prominent symptoms [23]. However, pediatric patients tend to exhibit more systemic symptoms like fever and fatigue [19]. This highlights the need for pediatric-specific diagnostic criteria and management strategies, tailored to address the unique presentation in children.
Furthermore, the variability in ECG and imaging findings underscores the necessity for a comprehensive and multifaceted diagnostic approach. Previous studies have emphasized the importance of ST-segment elevation as a diagnostic marker, which is consistent with our findings. However, the presence of normal ECGs in a significant proportion of patients indicates that reliance on a single diagnostic tool may be insufficient, reinforcing the need for comprehensive evaluations using multiple modalities. The elevated CRP levels observed in this study align with previous research that has highlighted the inflammatory nature of pericarditis. Monitoring inflammatory markers like CRP is crucial in differentiating pericarditis from other causes of chest pain and in guiding treatment decisions [9, 26]. This approach is supported by the literature, which advocates for the use of CRP as a reliable marker of inflammation in pericarditis.
This study has several limitations. The retrospective nature of the included studies may introduce biases, and key variables might have been omitted, limiting the comprehensiveness of the analysis. Significant heterogeneity observed in several outcomes reflects variability in clinical practice and patient populations across different studies. Future research should focus on prospective multicenter studies to provide more robust evidence on the clinical course and optimal management strategies for pediatric pericarditis.
Despite these limitations, our study provides valuable insights into the clinical presentation and diagnostic evaluation of pediatric pericarditis, highlighting the need for a comprehensive and standardized approach to diagnosis and management. The strengths of our study include a comprehensive search strategy, rigorous inclusion criteria, and a robust meta-analytic approach. To improve clinical outcomes, we recommend standardizing diagnostic criteria by implementing protocols for ECG interpretation, imaging evaluation, and inflammatory marker assessment. Early recognition of symptoms and timely initiation of anti-inflammatory therapy are crucial to prevent complications. Additionally, ensuring careful long-term follow-up for pediatric patients diagnosed with pericarditis is essential to monitor for potential chronic complications.






Comments (0)