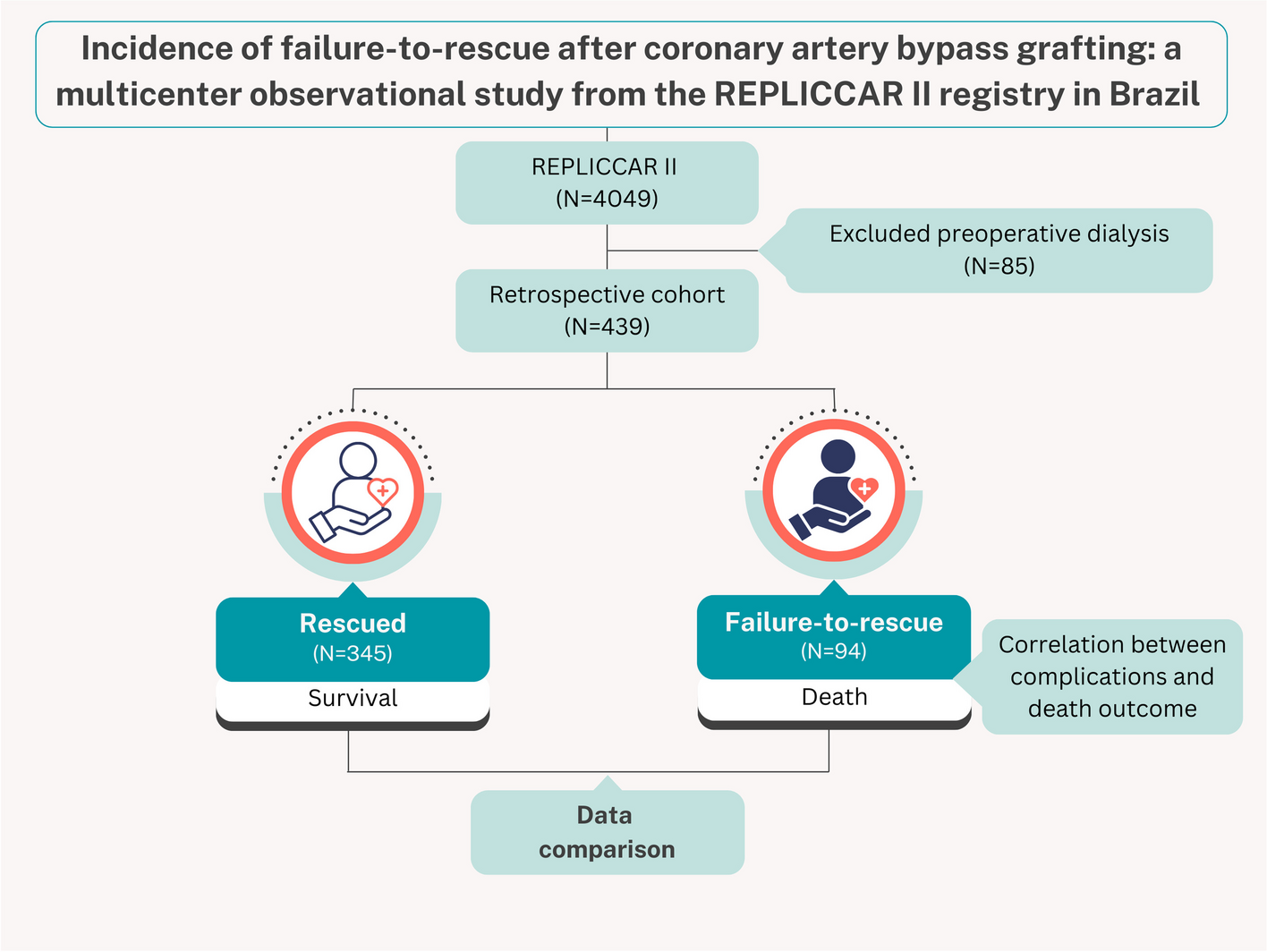
Our results indicate that the failure-to-rescue rate in the São Paulo database REPLICCAR II (21.41%, 94/439) is comparable to the rates reported in previous studies performed in other countries [7, 10, 15], confirming that observed mortality increases progressively according to the greater number of combinations of complications.
Failure-to-rescue emerges as a relevant metric in quality analysis, adding value to the known variables, mortality and morbidity, which are traditionally evaluated, providing an opportunity to evaluate the institution and its effectiveness in reversing hospital-acquired complications and preventing deaths. A low failure-to-rescue rate, despite a high incidence of complications, reflects a high-performance hospital team and adequate infrastructure. On the other hand, a high failure-to-rescue rate indicates the need for the hospital to readjust and reassess the clinical experience, as well as the institutional resources, to enhance patient care [7,8,9].
Currently, no consensus exists on the complications correlated with failure-to-rescue in cardiac surgery, and the heterogeneity of variables in the scientific literature is significant [7, 8, 10, 15, 16]. This study followed the method presented by The Society of Thoracic Surgeons (STS) [10], which will soon incorporate this new metric into its risk prediction calculator. However, it is important to emphasize that current risk scores are unable to monitor and update patient evolution as they evolve.
The inflexibility of current risk scores blinds healthcare professionals to the risk of their patients during hospitalization, which impairs the therapeutic decision-making process. In 2016, Ranucci et al. [17] proposed a classification strategy at two different times to update the indices according to the patient’s status. This strategy aims to address the frustration related to the attempt to stratify the risk of high-risk patients in cardiac surgeries and the discrepancy between the predicted and observed values. Such an approach can improve the performance of the outcome predictor scores. Furthermore, with technological advancements, it is desirable that healthcare applications and platforms, such as Kamay [18], Cardux [19], or the Prehab APP [20], could enable real-time, personalized, and predictive patient care, thus feeding into continuous improvement cycles [18,19,20,21]. Given this observation, we believe that the new metric of STS [10], associated with the strategy of reclassification of the patient’s risk score during the hospital stay [17], might be a valuable tool to reliably monitor the patient’s status. However, a study focused on this analysis should be carried out.
In our analysis, patients in the failure-to-rescue group had a higher predicted risk of mortality, acute kidney injury, reoperation, and prolonged ventilation as estimated by STS, compared with the Rescued group. In addition, age and sex were also a differential between groups, which represents that the population was potentially more complex. Previous studies have shown a correlation between advanced age of the patient and higher rates of failure-to-rescue [8, 15], as well as female patients [22] highlighting the knowledge gap surrounding the failure-to-rescue in the fragile and female populations. This finding underscores the challenge of accurately assessing a patient’s risk and strategically planning the procedure, as failure to identify factors related to the risk of these complications can culminate in a cascade of events leading to failure-to-rescue, mainly in hospitals [9, 23] with lower surgical volume [9, 23] or without teams aligned for high-performance care.
Comparing the results of this study and STS’s database [10], we observe a similar overall mortality rate, with 2.37% in our study and 2.6% in the STS. We attribute these outcomes to the REPLICCAR project’s emphasis on quality improvement through data-driven strategies [5, 6]. The rates of analyzed complications were also closely aligned, with 11.07% in REPLICCAR II and 12% in STS. Additionally, failure-to-rescue rates were also comparable between the studies, showing 21.24% and 21.41% respectively. Both datasets further demonstrate a trend: as complication combination increases, so does the failure-to-rescue rate, underscoring the impact of cumulative complications on patient outcomes across populations, even in different socioeconomic levels, countries, and healthcare context.
The quantification of healthcare quality reflects a constantly evolving challenge, especially regarding patients referred for high-risk cardiac surgeries. Value-based medicine has gained increasing prominence in society through the pay for performance model and the search for better outcomes for patients undergoing surgical procedures, which is already a reality in the Latin American scenario [24, 25]. Recognition and continuous efforts to reduce failure-to-rescue rates are challenges that emerge and stand out in the current literature and are closely linked to institutional competence.
This pioneering study in the Latin American scenario presents the failure-to-rescue in patients who had one or more complications after CABG, which is relevant as it alerts hospital managers, healthcare professionals, and especially patients about this metric’s potential to identify care difficulties, providing the opportunity to create strategies within the concepts of continuous improvement in cardiac surgery. Upcoming analyses should bring results on external validations of the new STS [10] calculator and comparisons of scores predicting the risk of failure-to-rescue by hospitals.
Study limitations
This study aimed to determine the current failure-to-rescue rate in São Paulo centers participating in REPLICCAR II. Due to ethical considerations, we did not analyze each institution separately, thus, the analysis may have been biased related due to variation in patient profiles, clinical experience, and available resources among the hospitals. As the failure-to-rescue rate is a metric used to evaluate hospital quality and care teams, future studies should include individualized analyses for each institution, allowing for the development of specific strategies for each center and/or care team.
Because of the heterogeneity of variable selection to characterize failure-to-rescue in cardiac surgeries [7, 8, 10, 15, 16], we followed the methodology proposed by the STS [10]. However, the authors warn about the importance of evaluating complications such as surgical wound infection in future studies, because the prevalence is divergent across countries and considerable in our reality [25,26,27]; however, these studies have been excluded from the calculator thus far.
In our analysis, we did not observe the combination of the four complications studied, and we believe that this fact is attributed to the small sample size. However, despite this limitation, our pioneering study in Brazil warns about the current scenario, which tends to underestimate low-risk patients and stiffens the risk prediction through scores that do not follow patient evolution. This can lead to unexpected clinical worsening, triggering unfavorable outcomes.






Comments (0)