
Remember me
Dear Editor,
Eccrine syringofibroadenoma is a rare adnexal neoplasm with varied clinical presentations but similar pathologic findings. The reactive form is associated with different diseases, including primary cutaneous amyloidosis. Amyloidosis cutis dyschromica is a rare type of cutaneous amyloidosis with generalised reticular hypo- and hyperpigmentation generally present since birth. To the best of our knowledge, the association between eccrine syringofibroadenoma and amyloidosis cutis dyschromica remains unreported.
An otherwise healthy 60-year-old man presented with a slowly progressive, asymptomatic red rash on both legs that started ten years ago. Examination revealed multiple erythematous plaques coalescing into cobblestone pattern symmetrically distributed on the dorsal, ventral and lateral surfaces of both legs [Figures 1a, 1b, 1c and 1d]. The patient also reported generalised reticular hyperpigmentation and hypopigmented macules on the trunk and extremities since birth [Figure 1e]. Hair, nails and mucosae were spared. Similar dyschromatosis was reported in his brother and father.

Export to PPT
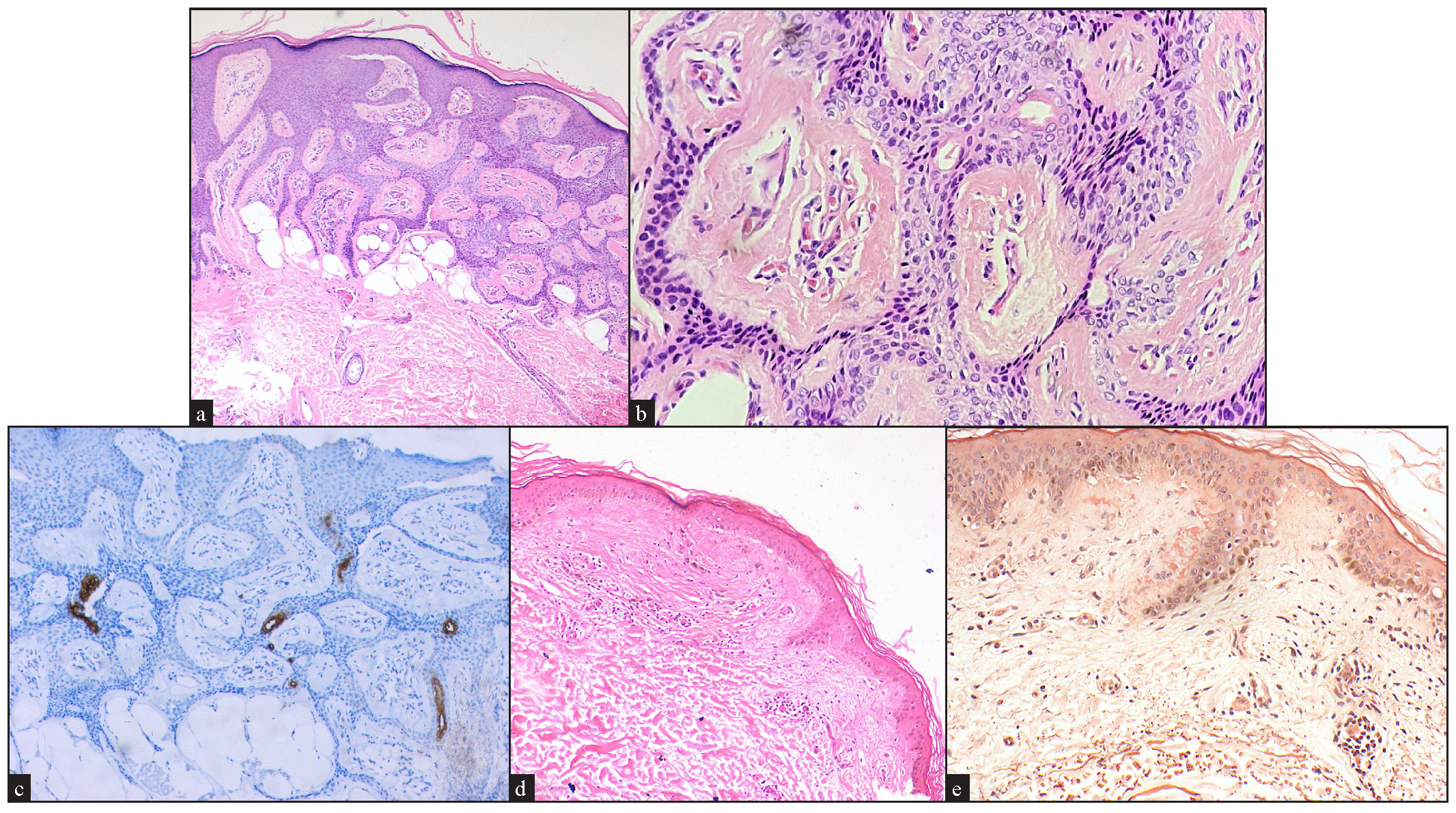
Histology from an erythematous plaque on the right leg demonstrated thin anastomosing epithelial cords and strands connected to the undersurface of the epidermis with ductal differentiation [Figures 2a and 2b]. Carcinoembryonic antigen highlighted the ductal parts [Figure 2c]. Histology from the background skin with dyschromatosis on the back of the patient revealed clumps of eosinophilic globules in the papillary dermis that showed positive Congo red staining [Figures 2d and 2e]. Based on the clinicopathological correlation, we made a diagnosis of reactive eccrine syringofibroadenoma in a patient with amyloidosis cutis dyschromica.
Export to PPT
Eccrine syringofibroadenoma is considered either a benign adnexal neoplasm, a hamartoma or a reactive eccrine epithelial hyperplasia. It is characterised by the proliferation of cords and strands of ductal epithelium connected to the undersurface of the epidermis.1 Histopathological differential diagnoses include fibroepithelioma of Pinkus, squamous cell carcinoma, pseudoepitheliomatous hyperplasia and follicular infundibular tumours [Table 1].2
Table 1: The histopathological differential diagnosis of eccrine syringofibroadenoma
Histopathological differential diagnosis Differentiating points Fibroepithelioma of Pinkus Reticulated interconnected basaloid epithelial strand with no ductal-like structures Squamous cell carcinoma Infiltrating nests of squamous epithelial cells with atypia Pseudoepitheliomatous hyperplasia Irregular strands of squamoid cells extending into the dermis which occurs in the setting of different occasions like chronic irritation, ulceration and chronic infections Follicular infundibular tumours Anastomosing strands with plate-like structure formation in the dermis and no ductal structuresFive types of eccrine syringofibroadenoma have been described: (1) solitary eccrine syringofibroadenoma, (2) multiple eccrine syringofibroadenoma associated with ectodermal dysplasia, (3) multiple eccrine syringofibroadenoma without associated cutaneous manifestations, (4) non-familial unilateral linear eccrine syringofibroadenoma and (5) reactive eccrine syringofibroadenoma. The clinical picture is variable, ranging from a single plaque to widespread red papules and nodules. Several sites may be affected, but the extremities are most commonly involved.1
Reactive eccrine syringofibroadenoma has been associated with multiple skin conditions, such as ectodermal dysplasia, venous stasis, nail trauma, chronic skin ulcerations, diabetic foot ulcer, burn scars, squamous cell carcinoma, leprosy, bullous pemphigoid, epidermolysis bullosa, erosive lichen planus, peristomal dermopathy, hyperkeratotic eczema, psoriasis, naevus sebaceous and primary cutaneous amyloidosis.1
The etiopathogenesis of reactive eccrine syringofibroadenoma remains controversial. Repeated damage, regrowth and tissue remodelling of the skin and its appendages, including eccrine ducts, were proposed as the cause in inflammatory and neoplastic skin diseases.3 Impaired keratinocytes differentiation and metabolism is another theory for the development of reactive eccrine syringofibroadenoma, supported by immunohistochemical studies that proved impaired cytokeratin expression in eccrine syringofibroadenoma.4
The course of a reactive eccrine syringofibroadenoma is mostly benign; however, malignant transformation has been reported. Treatment depends on the number and the site of the lesions. Retinoids, surgical excision, electrodesiccation, cryotherapy and ablative lasers have been tried with variable results.2
To the best of our knowledge, we have reported the first case of reactive eccrine syringofibroadenoma in the setting of amyloidosis cutis dyschromica. Amyloidosis cutis dyschromica is a rare subtype of primary cutaneous amyloidosis, characterised clinically by reticular hyperpigmentation with hypopigmented macules on the trunk and extremities. The pathogenesis of amyloidosis cutis dyschromica has been attributed to abnormal keratinocytes survival and differentiation, disturbed keratin metabolism and defective deoxyribonucleic acid repair which occur secondary to mutation in Oncostatin M Receptor, interleukin 31 receptor A and glycoprotein non-metastatic melanoma protein B genes.5
We suggest that the development of reactive eccrine syringofibroadenoma in amyloidosis cutis dyschromica may be attributed to abnormal differentiation signals in keratinocytes resulting in their ductal transformation.
Comments (0)