
Remember me


American households are surveyed as part of NHANES, a cross-sectional study designed to measure health, nutrition, and sociodemographic characteristics. Approximately 10,000 participants from 30 selected counties out of the about 3,000 counties in the U.S. take part in household interviews, physical examinations, and laboratory tests at a Mobile Examination Center (MEC) every survey cycle. The interview portion of NHANES encompasses inquiries pertaining to demographic, socioeconomic, dietary, and health-related topics.
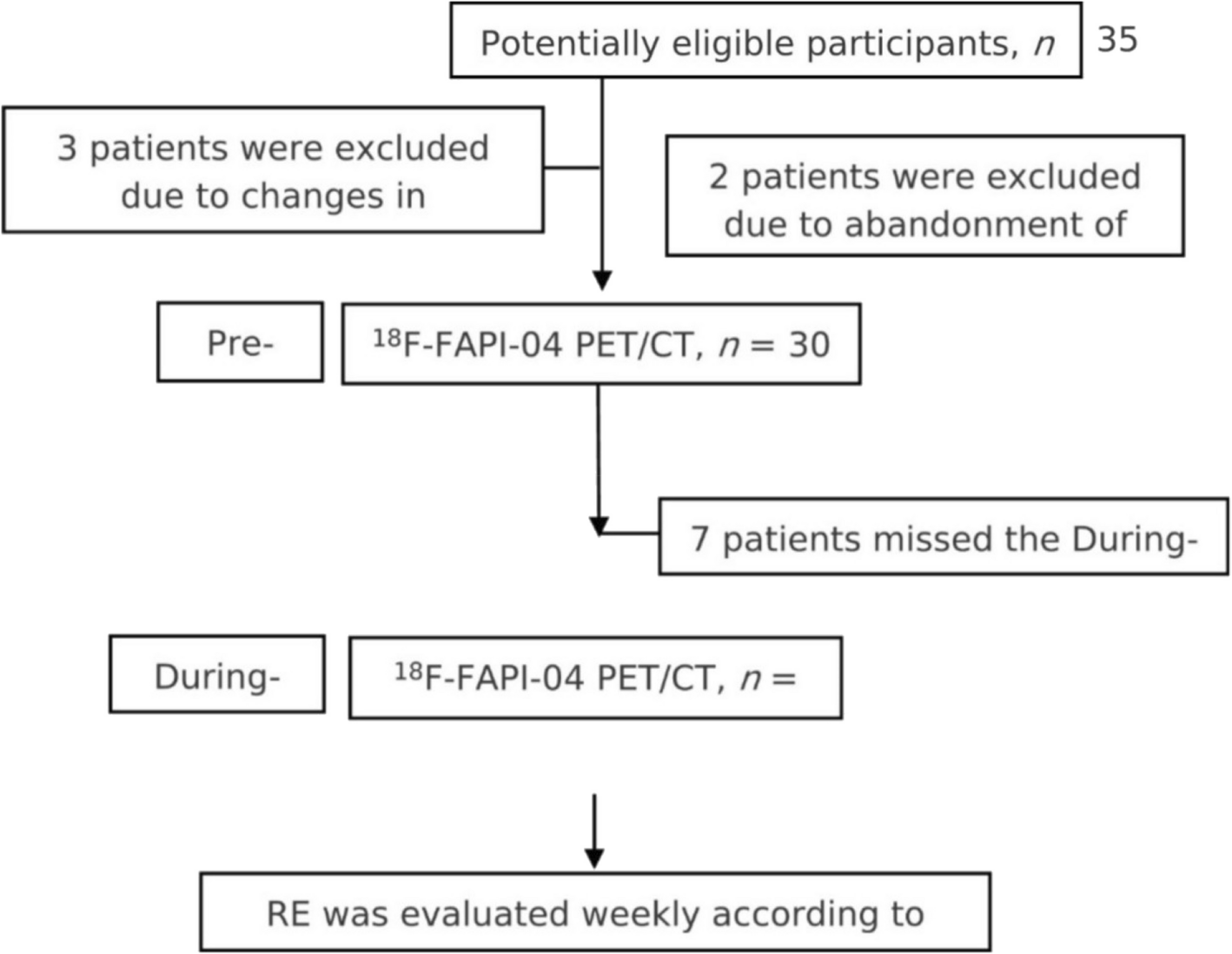
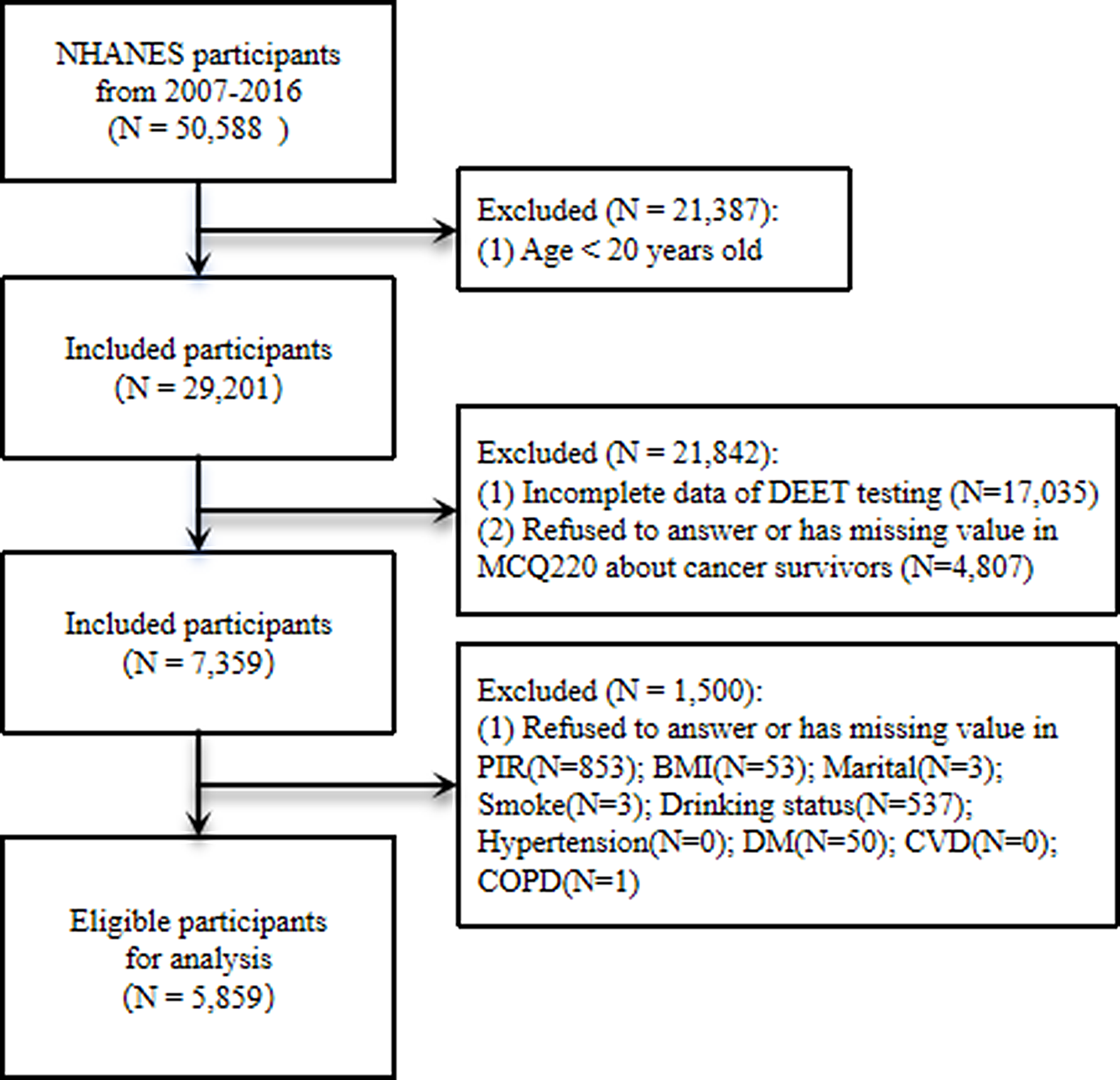
The examination component of this study encompasses a range of basic medical assessments, including blood pressure, hearing tests, oral health, grip strength, and various laboratory tests administered by qualified medical professionals, including certain radiological data. Data for this analysis was obtained from adult participants aged 20 and older in the NHANES spanning from 2007 to 2016. To be eligible for analysis, participants had to meet the following inclusion criteria: (1) completion of the Medical Conditions questionnaire, (2) availability of data on mosquito repellent use, and (3) assessment of baseline covariates. An analysis of 5,859 eligible patients was performed after excluding those with missing data (Fig. 1).
Fig. 1
Flowchart depicting the cohort included in this study
DEET assessmentDEET is commonly utilized as a highly efficient mosquito and tick repellent, predominantly through dermal contact. Upon application to the skin, DEET is absorbed into the systemic circulation. Subsequently, DEET undergoes rapid metabolism and is predominantly excreted via urine [15]. The major metabolite of DEET, DCBA, accounts for 83% of urinary excretion in the United States and is frequently employed as a specific biomarker for DEET exposure [16, 17]. This method uses online solid phase extraction coupled with high performance liquid chromatography-tandem mass spectrometry (SPE-HPLC-MS/MS) for quantifying DCBA, in 100 µL of human urine. Sample preparation begins with an over-night enzymatic deconjugation of the glucuronide-bound metabolites. On the second day, the four compounds being measured are concentrated via online SPE and then chromatographically separated from each other and from other urine biomolecules using reversed phase HPLC. The eluting molecular ions are converted to gas phase ions using Atmospheric Pressure Chemical Ionization (APCI) and then selectively filtered by mass-to-charge ratios at unit resolution. Select molecular ions are then fragmented with chemical induced dissociation (CID) and the resulting product ions are filtered at unit resolution before detection via an electron multiplier [18]. The aim of this study is to investigate whether DEET may have an impact on cancer survivors’ mortality, DCBA(µg/L) was stratified into four quartiles: Q1 [0.3352, 0.665], Q2 (0.665, 1.95], Q3 (1.95, 6.845], and Q4 (6.845, 382000].
Diagnosis of cancerA prior study evaluating the precision and reliability of NHANES self-reported cancer diagnoses revealed that medical documentation aligns well with self-reported information for the most prevalent cancer types [19, 20]. Participants’ cancer history is obtained from the “Medical Conditions” section of the NHANES database. Cancer survivors are distinguished by their response to the inquiry: “Have you received a diagnosis of cancer or malignancy from a medical professional?” Upon affirming this question, participants are classified as individuals who have experienced cancer.
Mortality ascertainmentNHANES public-use mortality files were linked to the National Death Index (NDI) using a probabilistic matching algorithm to collect mortality information for the follow-up group. Furthermore, the International Classification of Diseases, 10th Revision (ICD-10) was employed to ascertain the primary cause of death. All-cause mortality was defined as death resulting from any cause, encompassing cancer (C00-C97), cardiovascular diseases (I00-I09, I11, I13, I20-I51), cerebrovascular diseases (I60-I69), respiratory diseases (J40-J47), and other etiologies (residual). Cancer mortality is defined as death resulting from any malignant tumor during the follow-up period, which is measured from the baseline interview until the date of death or December 31, 2019 [21].
CovariatesBased on prior research on cancer survivor mortality rates, our study considers several potential factors that may influence the relationship between cancer survivor mortality rates and DEET. We collected and statistically analyzed various covariates, including age, gender (female, or male), race/ethnicity (Hispanic, Non-Hispanic Black, Non-Hispanic White, or Others), marital status (Married/Living with partner, Not married), Educational level (College or above, High school or GED, or Less than high school), poverty income ratio (PIR, < 1.3, 1.3–3.49, > 3.49), body mass index (BMI, < 25, 25–30, or > 30), smoking status (Former, Never, or Now), alcohol consumption (Former, Mild, Moderate, Heavy, Never), and health-related factors. The health-related variables considered in this study encompass hypertension, diabetes mellitus (DM including: DM, IFG, IGT, or No), cardiovascular disease (CVD including: No, or Yes), and chronic obstructive pulmonary disease (COPD including: No, or Yes), ascertained through physician self-reported diagnoses collected via standardized medical condition questionnaires during individual interviews. These variables were incorporated into our multivariable-adjusted model for analysis. Through statistical examination of these variables, our objective was to enhance comprehension of their influence on the association between cancer survivor mortality rates and DEET. By adjusting for these potential confounding variables, we aimed to improve the reliability and credibility of our research results.
Statistical analysisNHANES utilizes a sophisticated, multi-stage probability sampling design. Our study performed weighted analyses to correct for potential over- or under-representation within the sample, thus enhancing the generalizability of the findings to the U.S. population. We utilized R software, version 4.3.2 (version 4.3.2, https://www.r-project.org/), and the “survey” package to conduct our statistical analyses. We compared weighted baseline characteristics across groups to detect statistical differences among the DCBA quartiles. In this study, for the data of normal distribution, the continuous variable is expressed as the average value with standard error, and for the data of non-normal distribution, the continuous variable is expressed as the median with quartile range. Categorical variables were presented as counts and percentages. Group differences were evaluated using the weighted Student’s t-test, Mann-Whitney U test, one-way ANOVA, Kruskal-Wallis test and chi-square test, with statistical significance set at a two-tailed P-value < 0.05.
A multivariable Cox regression model employed to investigate the association between DCBA levels and overall mortality, cancer-specific mortality, and non-cancer mortality, adjusting for gender, age, marital status, ethnicity, education, PIR, BMI, hypertension, DM, CVD, and COPD. To investigate the potential non-linear association between the DEET and both all-cause mortality, cancer mortality and non-cancer mortality in cancer survivors, a restricted cubic spline (RCS) methodology was utilized. It was constructed using the “RMS” package in R. Knot positions were varied from 3 to 7, with the model exhibiting the lowest RCS information criterion value ultimately chosen, employing 3 knots. Inflection points were identified based on the RCS curve. Additionally, to gain further insights into the varying survival probabilities of cancer survivors based on urinary DCBA concentrations, a Kaplan-Meier (KM) curves was constructed using the " survey " package in R.
Subgroup analyses were conducted to assess the influence of confounding factors on the prevalence of cancer survivors associated with DCBA. We evaluated interaction effects by incorporating multiplicative interaction terms between DCBA and the respective subgroup variables.
Comments (0)