Primary liver cancer is the sixth most frequent cancer in the world and the third most common cause of cancer-related death worldwide [1]. This is a very rare case of HCC arising in the bone without a primary tumor in the liver.
When HCC tissue is found only outside the liver, the differential includes ectopic hepatocellular carcinoma with a primary tumor, hepatoid adenocarcinoma of bone origin, and bone metastasis of HCC without a primary tumor.
Ectopic hepatocellular carcinoma is defined as HCC arising from the liver parenchyma located in extrahepatic organs or tissues [3], Some case reports of ectopic hepatocellular carcinoma have been reported in patients without liver diseases such as viral hepatitis or cirrhosis, and the mechanism of carcinogenesis is believed to be different from that of HCC arising in normal sites, which is caused by biliary obstruction or vascular insufficiency of ectopic hepatocytes [4]. The sites of ectopic HCC have been reported to include the gallbladder, pancreas, omentum, retroperitoneum, and adrenal glands, and are thought to be most common around the liver and gallbladder [5]. Although there have been no reports of ectopic hepatocellular carcinoma arising in bone, a case of hepatocellular carcinoma with a primary site in the thoracic spine was reported based on the finding that bone marrow-derived cells are the origin of hepatocellular carcinoma [6]. The possibility that this case is also an ectopic hepatocellular carcinoma with a lumbar spine as the primary site cannot be ruled out.
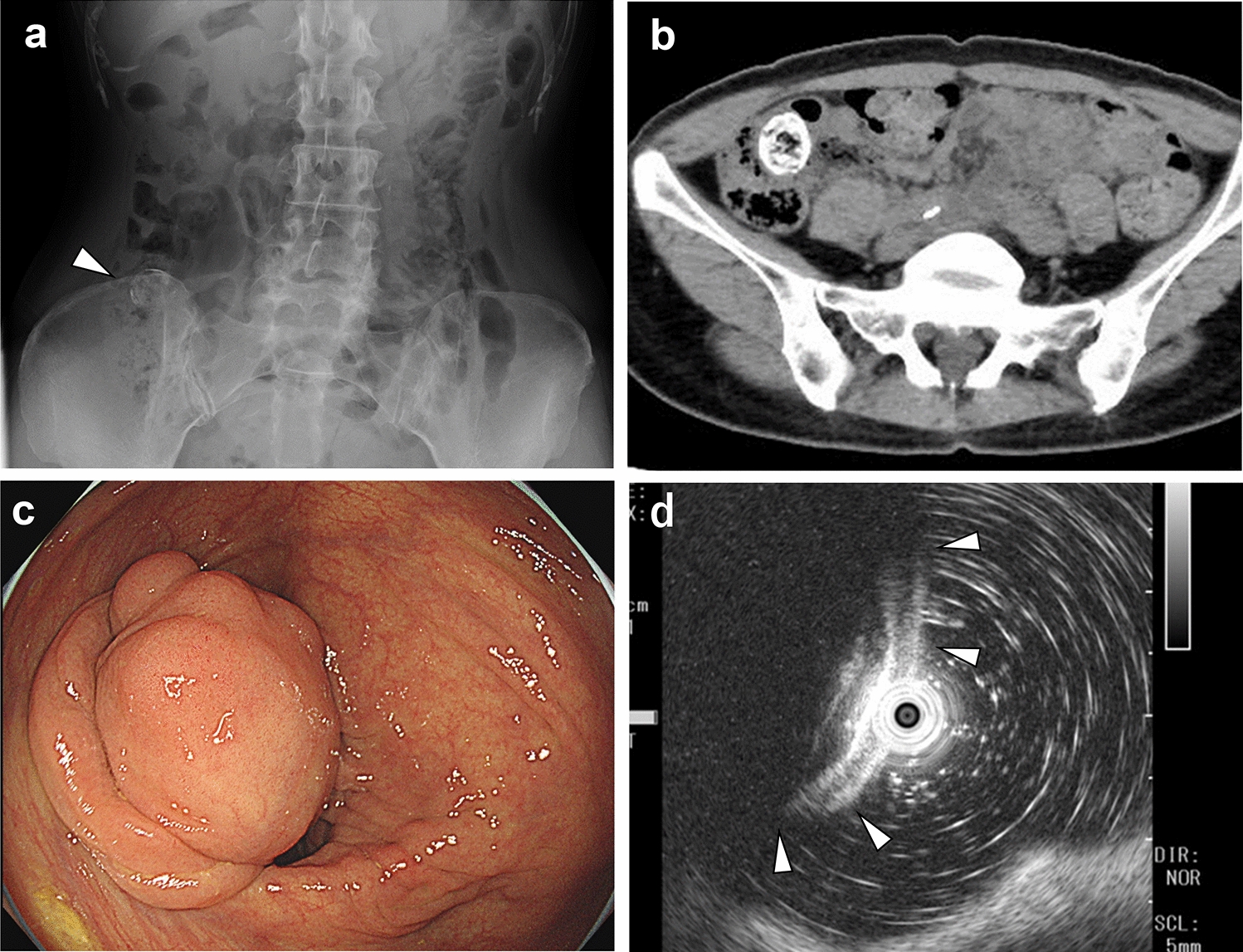
Hepatoid cell carcinoma is a tumor with features of hepatocellular carcinoma and adenocarcinoma arising in organs other than the liver [7]. It is known to occur in various organs, including the stomach, colon, lungs, pancreas, and uterus, but there are no reports of its occurrence in bones [8]. In this case, upper and lower gastrointestinal endoscopy revealed no neoplastic lesions in the gastrointestinal tract, and CT showed no neoplastic lesions other than in the lumbar spine. Pathologically, there were no findings suggestive of hepatoid adenocarcinoma, and the possibility of bone-derived hepatoid adenocarcinoma was considered unlikely.
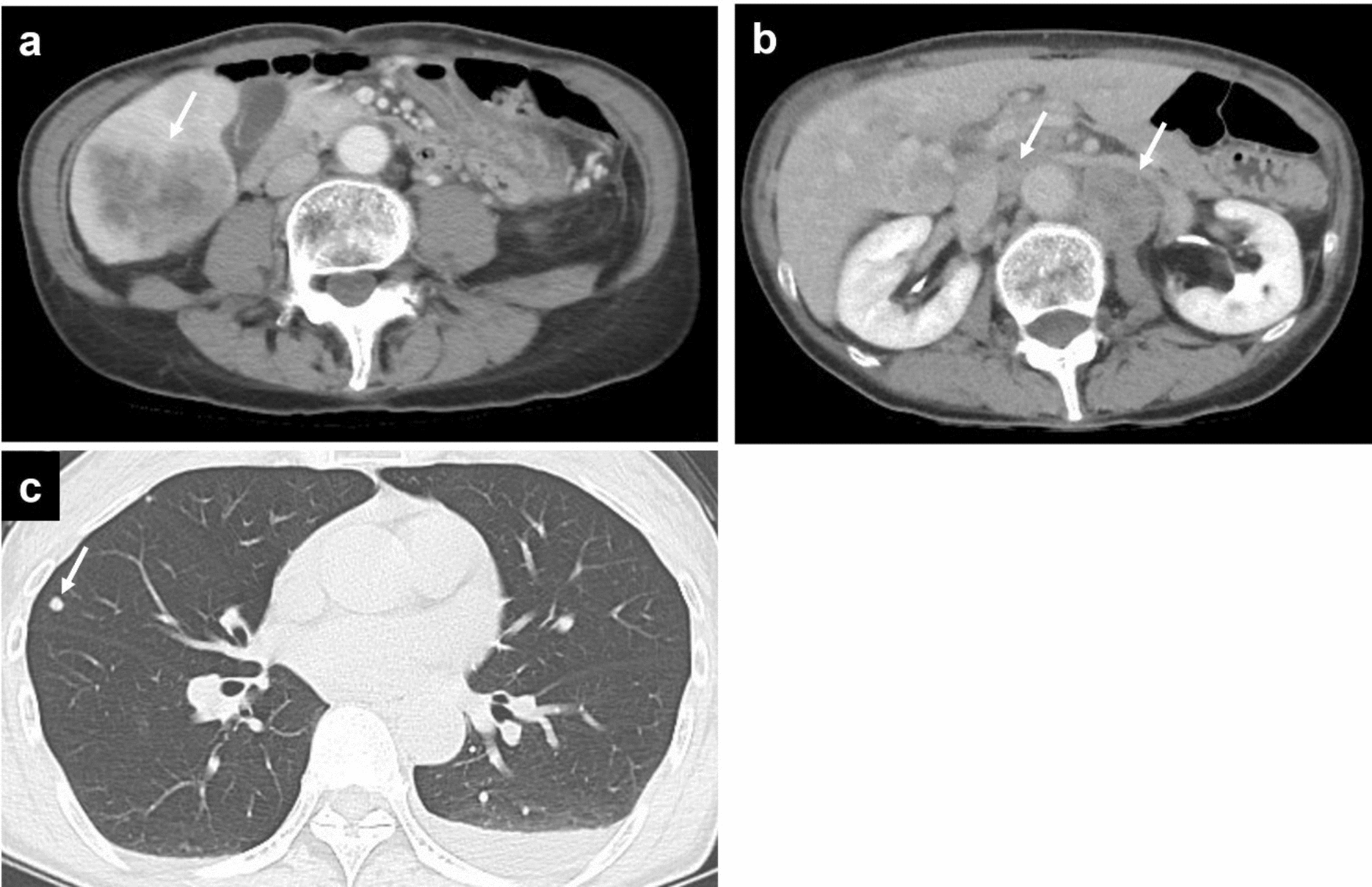
Next, we will discuss the case of a bone lesion being a metastatic lesion of hepatocellular carcinoma. The most common sites of HCC hematogenous extrahepatic metastasis are lungs (55%), abdominal lymph nodes (41%), bones (28%), adrenal glands (11%), and peritoneum (11%) [9]. The most common site of bone metastasis of HCC is the spine, followed by the pelvis and ribs [10]. In general, extrahepatic metastases usually occur in patients with advanced HCC [11]. Case reports of hepatocellular carcinoma with bone metastases but no primary tumor in the liver at the same time are very rare. I found the 15 cases of HCC in bone without a primary lesion in the liver by searching for previous reports. [12,13,14,15,16,17,18,19,20,21,22,23,24,25] (Table 2).
Table 2 cases of extrahepatic HCC without a primary lesion in the liver identified by literature search and the our caseThe absence of a primary tumor in the liver may be due to spontaneous regression of the hepatocellular carcinoma or metastasis from an HCC too small to be detected by imaging studies.
Spontaneous regression of cancer is estimated to occur in 1 case in 60,000 to 100,000 [26], and spontaneous regression of HCC is reported to occur in 1.1% to 2.4% of cases. The main mechanisms of spontaneous regression of hepatocellular carcinoma are necrosis due to ischemia and impaired blood circulation and activation of tumor immunity. The former, necrosis due to ischemia and impaired blood circulation, is thought to be caused by secondary nutrient vessel occlusion and poor angiogenesis due to catheterization such as abdominal angiography, damage to the lining of nutrient arteries, circulatory disturbance due to vessel occlusion, massive bleeding, impaired blood flow due to shock, and rapid tumor growth [27, 28]. The latter activation of tumor immunity has been attributed to the infiltration of inflammatory cells into the tumor, capsule, and surrounding tissues and the associated anti-tumor effects of elevated cytokines such as TNF-α. Triggers that have been cited include external factors such as blood transfusion, trauma, surgery, biopsy, drug involvement, abrupt alcohol cessation, alcoholism, smoking cessation [29], etc.
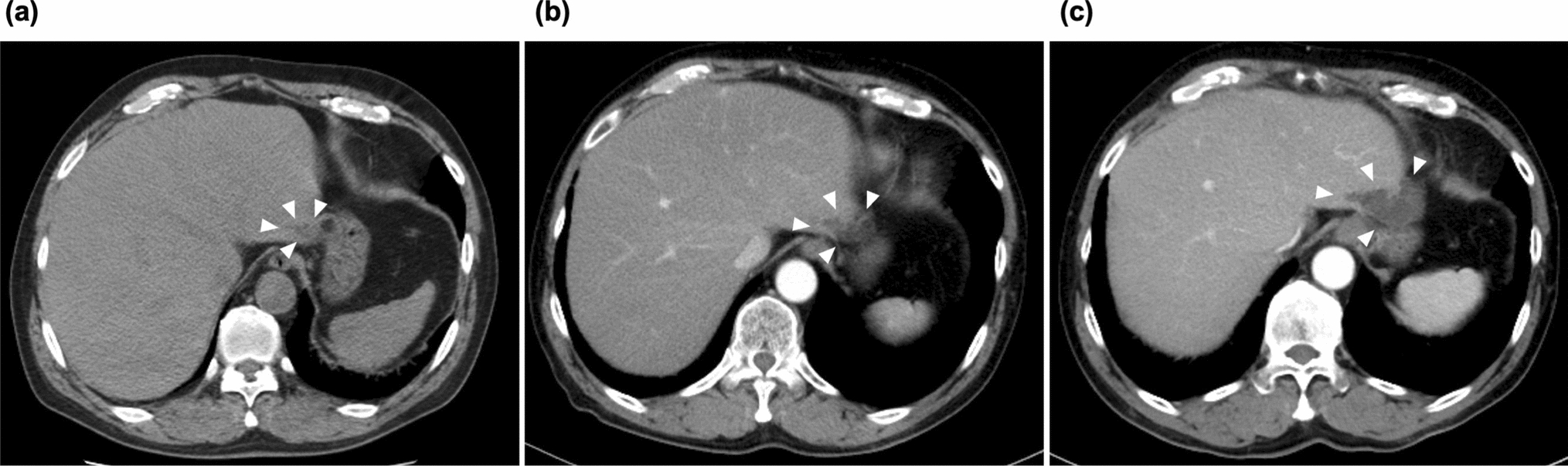
It is also possible that bone metastasis may have developed from HCC of a size that was difficult to detect in imaging studies. In the present case, bone metastasis occurred at the stage of microscopic HCC, which could not be identified by imaging at the time of initial diagnosis, and intrahepatic lesions may have disappeared or spontaneous necrosis may have occurred due to systemic drug therapy.
Treatment options for HCC include hepatectomy or liver transplantation, local therapy, chemoembolization, and systemic pharmacotherapy, but no standard treatment has been established for extrahepatic HCC without a primary tumor. The patient was diagnosed with stage cT0N0M1, cStageIVB, BCLC stage C. According to Western and Japanese guidelines [30, 31], first-line treatment in this situation is systemic drug therapy. Drug therapy includes the use of molecularly targeted agents and immune checkpoint inhibitors alone or in combination. Currently, durvalumab and tremelimumab, atezolizumab and bevacizumab, lenvatinib, and sorafenib are commonly used as first-line therapies for metastatic HCC. The patient underwent radiotherapy (39 Gy/13fr) to palliate symptoms of spinal cord compression due to bone metastasis, followed by systemic drug therapy with durvalumab and tremelimumab according to the guidelines.
The patient has been able to maintain CR for a long period of time, approximately one year, which may have been due to the combination of radiotherapy and ICI. In recent years, it has become clear that irradiation of malignant tumors elicits a specific anti-tumor immune response that enhances therapeutic efficacy. Irradiation of malignant tumors releases an immunostimulatory protein (HMGB1), which activates dendritic cells. In addition, T cells are activated when dead cancer cells are recognized and presented as cancer antigens through phagocytosis by dendritic cells [32]. The PD-1 receptor is an immune checkpoint receptor expressed on the surface of activated T cells that induces peripheral immune tolerance by binding to PD-L1 [33, 34]. Radiation induces PD-L1 expression in cancer cells and immune tolerance. This indicates that irradiation activates anti-tumor immunity, while at the same time the tumor reinforces immune escape mechanisms [32]. Thus, the combination of radiotherapy and PD-1/PD-L1 inhibitors is expected to enhance the therapeutic effect. On the other hand, CTLA-4 is an immune mechanism regulatory molecule expressed on the surface of activated T cells and constitutes an inhibitory pathway called the immune checkpoint; blocking CTLA-4 has been reported to enhance antitumor immunity [33, 34]. Based on the above, we believe that the combination of radiotherapy and the immune checkpoint inhibitors durvalumab and tremelimumab has suppressed tumor growth and maintained CR over the long term.


Comments (0)