
Remember me







All analyses were conducted with the German IQVIATM LRx database, which includes longitudinal patient-level prescription data of patients with statutory health insurance (SHI) [1]. The IQVIATM LRx database accesses nationwide pharmacy data collection centers that process prescription data for all German patients within the SHI system for reimbursement purposes. It is based on computerized records derived from pharmacy coding centers for public sick fund prescriptions (no private or cash prescriptions are covered), and in 2021 it covered approximately 80% of the total SHI prescription amount in Germany [10]. All patient information is fully anonymized by the data provider in accordance with data privacy laws. The de-identified patient-level data include dispensed drugs (e.g., brand, substance, package size, and product form) and associated information (e.g., specialty of prescriber, region identifier), as well as patient-level information such as patient age and sex. The collected data contain all Anatomical Therapeutic Chemical [] codes and prescriber specialties, including outpatient centers and authorized physicians in hospitals; therefore, the database provides a holistic view of outpatient treatments received by a patient. Finally, this database has been used effectively in previous studies on persistence [11, 12].
Study Design and CohortThis study is a non-interventional, retrospective, observational cohort study of German longitudinal prescription data. Included patients were statutory insured, 18 years or older, and received at least one prescription of tafamidis 61 mg between March 1, 2020 and August 31, 2022 (index period). Treatment adherence was analyzed in patients with at least two tafamidis 61 mg prescriptions during the index period.
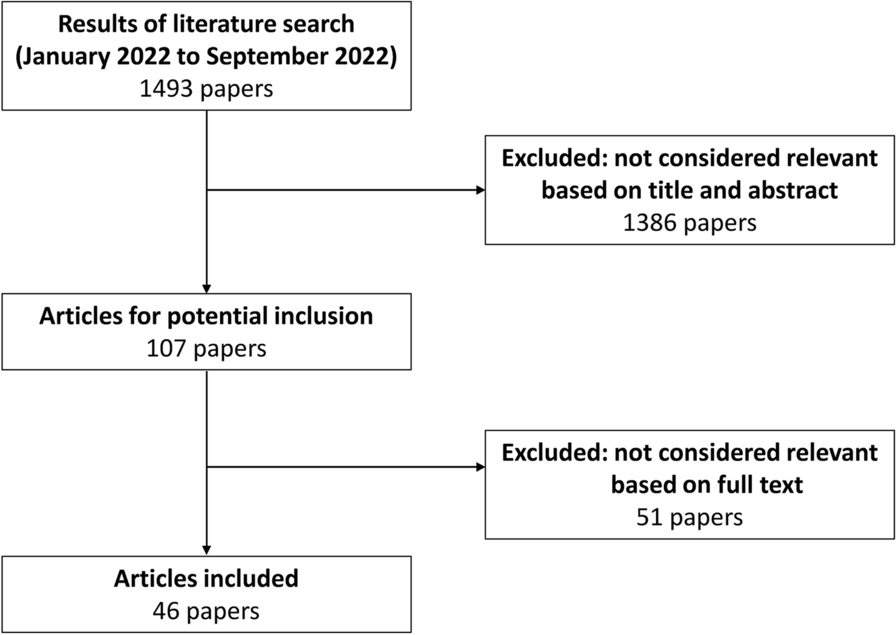
Patients included in the persistency analysis were sampled up to April 30, 2022, to allow for sufficient time to collect data on therapy. The selection of study cohorts for the different analyses is shown in Fig. 1.
Fig. 1
Selection of study patients for adherence and persistency analysis
Ethical ApprovalThe database used for this study includes only anonymized data in compliance with the provisions set forth in the applicable data protection laws. German law allows the use of anonymous electronic medical records for research purposes under certain conditions. In accordance with this legislation, it is not necessary to obtain informed consent from patients or approval from a medical ethics committee for this type of observational study that contains no directly identifiable data. Since all patients were only queried as aggregates and no protected health information was available for queries, no institutional review board approval was required for the use of this database or the completion of this study. IQVIA was contracted by Pfizer in connection with this study. Pfizer did not have permission to access the IQVIATM LRx database at any time during the study, but rather received aggregated results from the database.
Outcomes and Analysis DetailsThe primary objective of this study was to describe tafamidis 61 mg treatment patterns (i.e., treatment initiation, days of supply, adherence rates, and persistence) among patients with ATTR-CM. The secondary objectives were to analyze demographic characteristics of patients, such as patient age and sex, and to evaluate concomitant medications of patients dispensed prescriptions of tafamidis 61 mg QD.
In this study, the following analyses were conducted: (1) adherence analysis using the modified medical possession ratio (mMPR) and using the proportion of days covered (PDC) method; (2) concomitant medication analysis using McNemar’s test to compare medication prior to and during tafamidis 61 mg treatment; and (3) persistency analysis using the Kaplan–Meier method.
All three analyses utilized IQVIATM LRx data collected up to August 2022. The baseline patient characteristics were assessed descriptively. Adherence was analyzed by using two methods: the mMPR (calculated as the sum of the days’ supply for all prescription fills in the time period divided by the number of days in the time period), which allows for stockpiling so that adherence can go over 1, and PDC (calculated as the sum of days covered over the time period divided by the number of days in the time period), in which patients are classified as adherent based on mMPR/PDC greater than or equal to 80%. Mean, median, standard deviation (SD), and 25th and 75th percentiles were additionally calculated for both methods.
Concomitant medication use was analyzed using the McNemar’s test to compare patient numbers before the first tafamidis 61 mg prescription and during tafamidis 61 mg treatment.
Persistency was calculated using the Kaplan–Meier method allowing for both 90-day and 60-day prescription gaps. A subcohort of these patients was observable for at least 12 months after the first tafamidis 61 mg prescription and used as sensitivity analysis. P values < 0.05 were considered statistically significant. Analyses were carried out using SAS version 9.4 (SAS Institute, Cary, NC, USA).
Comments (0)