
Remember me
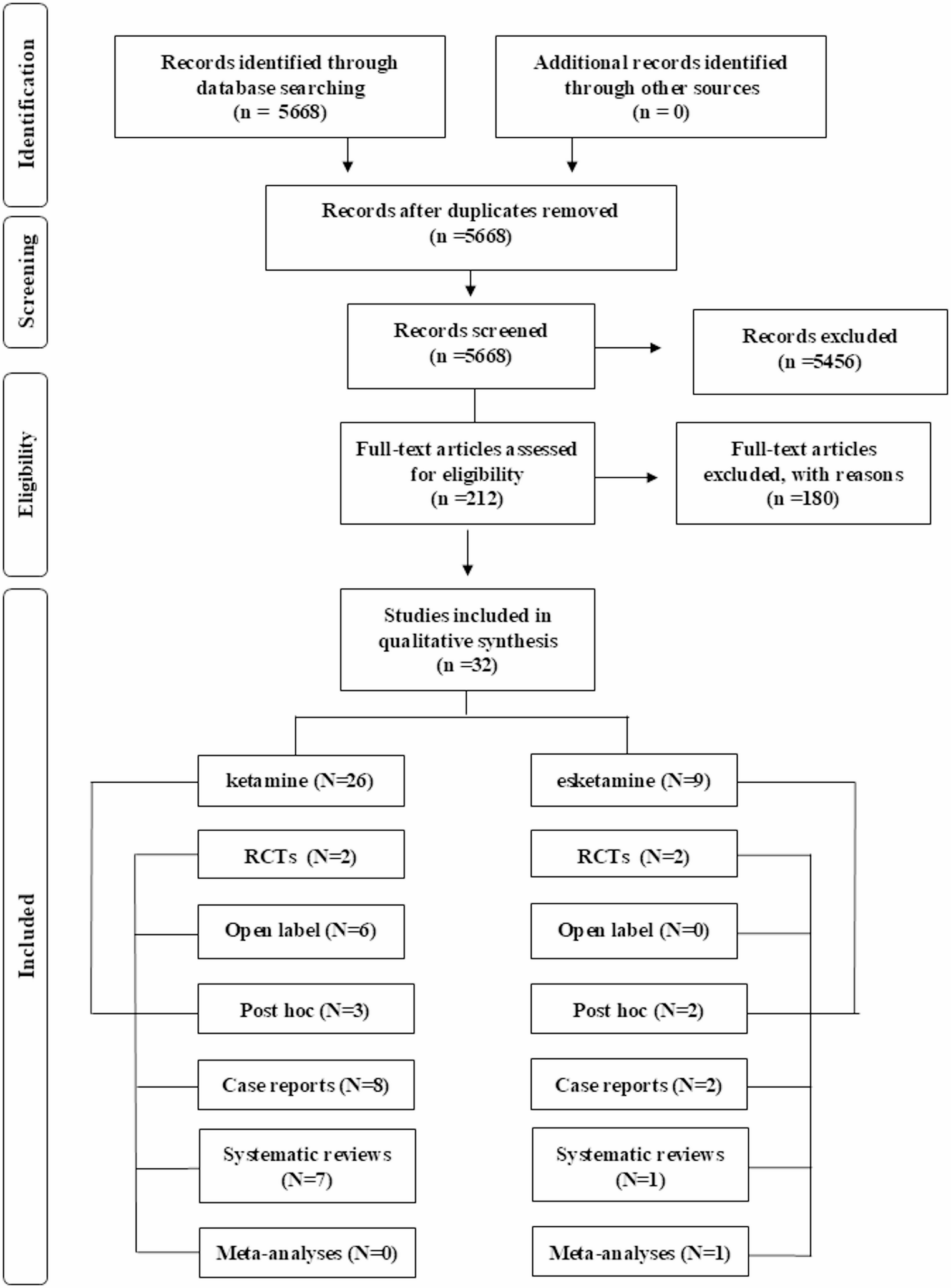

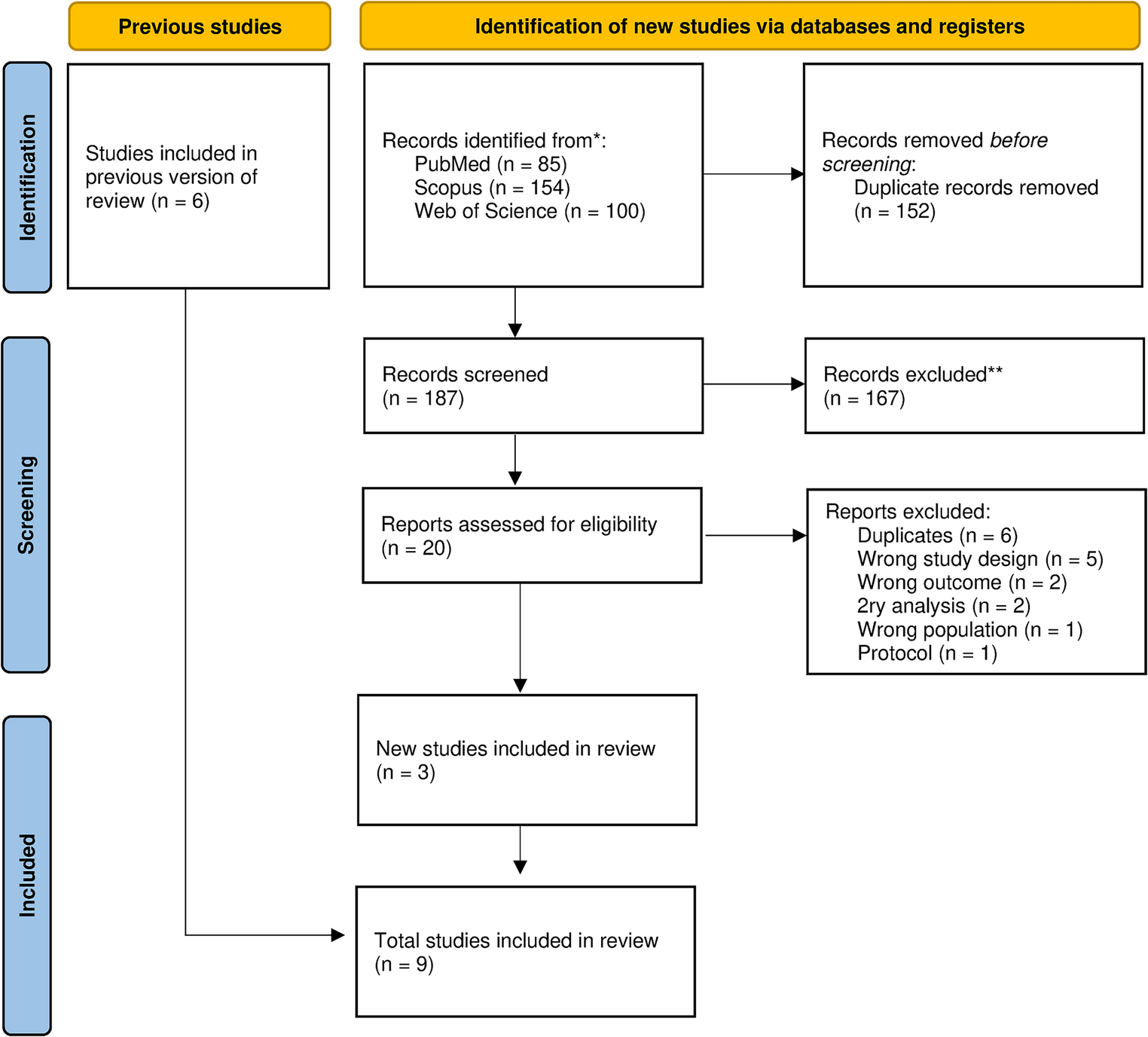
We identified a total of 66 reports (n) that related to 41 individual studies (t) and evaluated 30 different interventions (i). We included 12 RCTs in the meta-analysis, 36 studies for the quantitative synthesis, and 22 reports to investigate families’ experiences with interventions, of which 10 reports provided qualitative data and 14 reports quantitative data regarding acceptability, satisfaction, and usefulness of the interventions. The flow diagram demonstrates the study selection process and reasons for excluding certain studies.
 Study characteristics and quality ratings
Study characteristics and quality ratingsMost studies were conducted in the United States (51%; 21/41), five in the United Kingdom (12%; 5/41), four in Germany (9%; 4/41), and the rest in Finland, Australia, Greece, Ireland, Sweden, Canada, Spain, China, and Iran. Children’s ages in the study samples ranged from 3 to 19 years (mean age of 11.4 years). More details about sample characteristics per study, including age, gender, and ethnicity of parents and children, are provided in Table S1 in the supplements. Twenty-seven studies included a control group (65%; 27/41), of which 18 were RCTs, five non-randomised control trials and four feasibility or pilot trials. Eight studies (19%; 8/41) had a single-group design providing quantitative descriptive statistics, and ten studies (24%; 10/41) involved qualitative research methods (two of which were part of an RCT).
All reports were independently assessed by two researchers (HM and AML) using the MMAT. A total of 1491 ratings were made by each assessor, and in 68 cases (4%), further discussions and control checks were needed to find an agreement (the MMAT ratings sheet and cases that required more discussion is provided in the supplements). Over one-third of the papers (38%; 26/66) had a high-quality rating of four or five stars (80–100% of the items scored as ‘yes’), 28% (19/66) were given a medium-quality rating of three stars (60% quality score), and 28% (19/66) had a low rating of one or two stars (20–40% quality score). Two papers were of very low quality (i.e., no stars). A high-quality rating of 80–100% was received by 44% of the RCTs (8/18), 50% of the qualitative and mixed method papers (2/4), and 20% of the non-randomised trials (1/5) and 66% (4/6) of the descriptive quantitative studies. Table 1 presents an overview of the study characteristics.
Table 1 Overview of included trials and studiesTypes of whole-family interventions and componentsMost interventions (46%; 14/30) addressed parental depression or substance misuse (30%; 9/30). The remaining interventions addressed families affected by anxiety disorders, bipolar disorders, or multiple disorders. Children needed a diagnosis or symptoms of mental illness to be included in seven of the interventions. The majority of the interventions (86%; 26/30) were outpatient or community-based, one was inpatient, and three used a combination of settings. Most interventions were manualised (90%; 27/30) and had a duration of 3 weeks up to 6 months (80%; 24/30). Two interventions were less than 1 week long, two were up to 9 months, and two were unspecified or open-ended. Fifteen (50%; 15/30) of the interventions worked with families individually, thirteen (43%; 13/30) interventions were delivered to groups of families, and two (6%; 2/30) interventions included both individual and group components.
We regarded interventions as having a family component when they included sessions or activities where members from at least two different levels (e.g., parent vs child level) in the family system were involved. Three interventions (10%; 3/30) had no family component where parents and children received treatment separately. Eight interventions (26%; 8/30) consisted of only family components, where all sessions involved a minimum of parents/caregivers and their children. Other interventions offered a combination of parent or child-only components with whole-family components. Intervention programmes differed in terms of who they involved as part of the family, three interventions (10%; 3/30) included parent–child dyads (mostly mothers), and another three (10%; 3/30) involved parent(s) and one child. The remaining interventions (70%; 21/30) stated that siblings, partners, and other family members were invited to take part. Table 2 gives a summary of the intervention characteristics and Table 3 provides an overview of the family components per study and which family members had been involved.
Table 2 Summary of all included interventionsTable 3 Overview of family componentsIntervention components were grouped into five higher level component characteristics: (1) structural components, (2) components from psychotherapeutic frameworks, (3) skills training, (4) psychoeducation, and (5) building resources. Twenty-four of the 30 interventions (80%; 24/30) included one or more of the identified structural components, although it varied what structural components programmes included.
All interventions delivered regular sessions, with two interventions being open-ended and the rest following a fixed schedule. Approximately one-third of the interventions (30%; 10/30) set homework tasks or encouraged family members to practise between sessions. Some interventions (30%; 9/30) facilitated parent–child interactions by stimulating parents to spend quality time with their child or by creating positive parent–child moments in the sessions. Relatively few interventions included an assessment (40%; 12/30) or goal setting component (20%;6/30). Most interventions (76%; 23/30) drew on one or more psychotherapeutic frameworks, such as cognitive behaviour therapy or systemic family therapy. The most common frameworks were multi-family or group therapy (46%; 14/30), and cognitive behavioural therapy (50%; 15/30). Many also contained elements of play or creativity (30%; 9/30), such as hand puppets (ID-n:118) and drawing (ID-n:67).
All but one intervention, namely Multiple Family Therapy (ID-n: 205, 211), contained one or more skills training components. The majority of interventions taught problem-solving and coping skills (76%; 23/30) such as relaxation and breathing exercise; communication skills (67%; 20/30), and/or parenting skills (60%; 18/30). Some interventions (30%; 9/30) specifically focused on supporting families with talking about parental mental illness in the family.
Most interventions (90%; 27/30) included one or more psychoeducational components, with the majority (70%; 21/30) providing psychoeducation on mental illness. Almost half of the interventions (50%; 15/30) provided psychoeducation on the impact of parental mental illnesses on children and other family members.
Increasing support and resources for families, such as developing a family care plan or strengthening the family’s network, was provided by fewer than half of the interventions (46%; 14/30). Some interventions aimed to build support networks for children (36%; 11/30) and parents (26%; 8/30) by identifying sources of support (ID-n:10) and encouraging positive friendships (ID-n:143). Interventions also linked and signposted participants with other potentially helpful services (40%; 12/30), such as social services (ID-n:123). A detailed overview of the intervention components can be found in the Supplement materials 2.
Effectiveness of whole-family interventionsThirty-six independent studies provided quantitative data on child, parent, and family outcomes. Table 4 provides an overview of the results for the included studies per outcome category. Of the 36 studies, 28 studies (77%; 28/36) assessed changes in child mental health outcomes, 15 (41%; 15/36) in parental mental health outcomes, and 27 (75%; 27/36) in family outcomes. We focussed on the following child, parent, and family outcomes: child internalising problems (i.e., anxiety, depression, and suicidality), child externalising problems (i.e., behavioural problems, conduct problems, and attention-deficit hyperactivity disorder), parent symptoms of mood and anxiety disorders (here summarised as internalising), parental substance abuse, other parental psychological symptoms (i.e., psychological distress and global functioning), family functioning (i.e., spouse relationship, sibling relationship, family communication, family conflict, family times, and routines), parenting (i.e., parenting stress, parenting sense of competence, parenting skills, parenting style, and child abuse), and assessments of the parent–child relationship (i.e., communication, and parent–child conflict or observation of interactions).
Table 4 Overview of results for intervention outcomes per studyChild internalising outcomesTwenty-seven studies (75%; 27/36) assessed changes in children’s internalising symptoms (27%; 10/36), including depression (41%; 15/36) and anxiety symptoms (19%; 7/36). Of these 27 studies, five studies (18%; 5/27) found no intervention effects, nine studies (33%; 9/27) reported mixed findings and 13 studies (48%; 13/27) reported significant post-intervention effects of reduced internalising symptoms in children. Studies reporting no intervention effects were small pilot studies (ID-t: 2, 22, 25). Of the 13 studies that indicated any positive intervention effects, 8 studies reported effect sizes of which the majority (t = 5) were small-to-medium-effect sizes (d = 0.22–0.42). Studies reporting large-effect sizes (d = 0.95–1.58) were also either small pilot or feasibility trials (ID-t: 7, 16, 26). Seven of the 13 reportedly ‘effective’ studies involved an active control condition of which only two (7%; 2/27) reported significant ‘time × group’ effects (ID-t: 15, 35). Three studies that reported significant time effects but no ‘group × time’ effect involved control groups that received a short intervention containing psychoeducational lectures for parents (ID-t: 1,3,6). For the other four studies, three control groups received treatment as usual and one received enhanced care containing six additional psychoeducational sessions. Nine studies reported mixed findings (33%; 9/27), where findings differed between reporters (t = 5; i.e., parent, clinician, and child), type of self-report measure used (t = 4), or effects were temporary or disappeared after controlling for baseline measures. In terms of reporter differences, we found that parents and clinicians tended to report greater changes in children’s internalising levels compared to children themselves.
Child externalising symptomsFewer studies (50%; 18/36) assessed children’s externalising problems. Eight studies (22%; 8/36) measured changes in behavioural and externalising symptoms, six (16%; 6/36) assessed conduct symptoms, including aggressive behaviour, three studies (8%; 3/36) measured changes in children’s hyperactivity levels, and one study (2%; 1/36) assessed levels of drug use. Of the 18 studies assessing any type of externalising symptoms, eight studies (44%; 8/18) reported some intervention effects, eight studies (44%; 8/18) found no effects and two studies (11%; 2/18) reported mixed findings, where the results differed depending on the scale used (CBCL vs YSR) and the respective reporter (child vs parent). Of the eight studies reporting some form of intervention effect, three studies did not provide descriptive statistics or outcomes of statistical tests (ID-t 24, 26, 28). Five studies were small pilot or feasibility trials (ID-t 2,16, 21, 23, 26) of which three studies reported small-to-moderate-effect sizes (d = 0.39–0.62) and two reported large-effect sizes (d = 0.70–0.95); however, sample size in these studies were small.
Parental mental health outcomesFifteen studies assessed any parental mental health outcomes. For internalising symptoms (t = 11), three studies (27%; 3/11) reported significantly better parental internalising outcomes in the intervention group compared to the control group. Six studies (55%; 6/11) reported positive changes over time and two studies (18%; 22/11) reported mixed findings, where findings differed by measurement or time of follow-up assessment. Four of these studies reported effect sizes, which ranged between d = 0.71 to d = 1.06, thus indicating moderate-to-large intervention effect. However, only one of these studies (ID-t:31) had a high-quality rating and included a control group. For parental substance abuse, most studies (80%; 4/5) reported mixed findings and none reported effect sizes. One study (ID-t:20) reported positive intervention effects for substance abuse in both the treatment and the TAU group, but the effects differed for certain subgroups, which was linked back to initial referral reasons. Studies assessing other parental mental health outcomes (t = 4) reported positive changes; however, they found no significant ‘group x time’ differences (t = 1), no control group was present (t = 3), and only two studies reported effect sizes (d = 0.86 and d = 0.93) which albeit large were both small feasibility studies without a control group.
Family outcomesA total of 27 (75%; 27/36) studies assessed family outcomes relating to family functioning (55%; 15/27), parenting behaviour (51%; 14/27), and parent–child relationship (33%; 9/27). For family functioning, five studies (33%; 5/15) reported any positive changes but only one found significant ‘group × time’ effects. Nine (60%; 9/15) studies reported mixed findings, and two (13%; 2/15) reported no effect for family functioning. Six studies (37%; 6/16) reported positive changes in parenting, eight (50%; 8/16) reported mixed findings, and two (12%; 2/16) reported no effects in parenting. For changes in parent–child relationships, two studies (25%; 2/8) reported positive ‘group × time’ changes, three reported mixed findings (37%; 3/8), and three (37%; 3/8) observed no changes in the parent–child relationship. On a few occasions, findings were in favour of TAU, for instance in Project Hope (ID-t:22, families receiving TAU indicated better family communication); and in Kanu (ID-t:15), the researchers observed that levels of parental rejection were lower in the control group. Only two studies (ID-t:21 and 23) reported effect sizes for family outcomes, which suggested moderate-to-large effects for family functioning (d = 0.57–1.03) and small-to-moderate effects for parenting behaviours (d = 0.03 to d = 0.52).
Meta-analysisFor the meta-analyses, we extracted 63 effect sizes from 12 studies (t) with a pooled sample size of n = 1298 (nt = 681 participants in treatment condition and nc = 617 in control conditions). We conducted multiple analyses to distinguish between different levels of child and parent outcomes as well as type of reporter (parent/child) and four different times of follow-up assessment. The below outcomes are reported in ranges to reflect outcomes from the main (ga) and the sensitivity analysis (gb).
Child mental health outcomes reported by childrenStudies with short-term follow-ups (t = 4) indicated small intervention effects for child internalising symptoms ranging between ga = − 0.27 (95% CI: − 0.53,0.00; p = 0.050) and gb = − 0.17 (95% CI: − 0.46, 0.13; p = 0.27). Similar trends (t = 10) were reported for internalising symptoms assessed between 6 and 10 months post-intervention ga = − 0.18 (95% CI: − 0.55; 0.20, p = 0.35) and gb = − 0.20 (95% CI: − 0.55, 0.16; p = 0.27). These small intervention trends decreased further in studies (t = 4) with longer follow-up times at assessment (10 to 18 months: ga = − 0.05; 95% CI: − 0.27, 0.18; p = 0.69 and gb = − 0.02; 95% CI: − 0.28, 0.25; p = 0.91; and 18 + months: ga = − 0.03; 95% CI: − 0.22, 0.15; p = 0.73 and gb = − 0.04; 95% CI: − 0.15, 0.22; p = 0.71). The forest plots (see Fig. 1 and Figs. S2–S8 in supplements) show that only three studies [11,12,13] consistently reported reduced internalising symptoms, while the remaining studies showed no significant treatment effects. Heterogeneity levels were small-to-medium across all meta-analyses, apart from one, where I2 = 87.12%–85.51% and H2 = 7.76–6.90 (see Figs. S1–S8 in supplement materials for all time-points and the sensitivity analyses).
Fig. 1
Forest plot child internalising outcomes reported by child at 0–6 month follow-up (a)
Child mental health outcomes reported by parentsSix studies included data on parent-reported internalising symptoms of children and were included in the following models. Pooled effect sizes ranged between ga = − 0.10 (95% CI: − 0.52, 0.33; p = 0.66) and gb = − 0.05; (95% CI: − 0.32, 0.21; p = 0.70) for studies with short-term follow-up assessments (see Fig. 2 and Figs. S9 and S10 in the supplements). Meta-analyses of studies reporting medium-term outcomes (t = 5) indicated slightly larger, yet small pooled effect sizes ranging between ga = − 0.16 (95% CI: − 0.33, − 0.02; p = 0.08) and gb = − 0.18 (95% CI: − 0.36, − 0.01; p = 0.04) at 6–10 months follow-up and ga = − 0.22 (95% CI: − 0.65, 0.22; p = 0.34) to gb = − 0.17 (95% CI: − 0.50, 0.16; p = 0.30) between 10 and 18 month follow-up (Figs. S11–S14). Only three studies reported outcomes for long follow-up assessments (See Figs. S15 and S16), of which one study reported significant findings [14]. Heterogeneity levels were high in all meta-analyses including studies with long-term follow-up assessments (I2 = 72.32%–89.43% and H2 = 3.61–9.46). See Figs. S9–S16 in supplement materials for all time-points and sensitivity analyses.
Fig. 2
Forest plot child internalising outcomes reported by parents at 0–6 month follow-up (a)
We did not conduct meta-analyses for child externalising symptoms as only three trials reported data for child externalising symptoms, of which only one [17] reported significant findings.
Parent mental health outcomesSix studies reported parental mental health outcomes, of which five reported on medium-term outcomes post-intervention (see Figs. S19 and S20), and the meta-analysis indicated small, non-significant effect sizes ranging between ga = − 0.14 (95% CI: − 0.35, 0.07; p = 0.19) and gb = − 0.16 (95% CI: − 0.36, 0.05; p = 0.14). Of the six studies, only one [18] reported significant short-term (3 months) and long-term (20 months) intervention effects of reduced depression symptoms in parents (see Figs. S17, S18, S23 and S24). Overall, the findings suggest small-to-no treatment effects for parent mental health outcomes. Heterogeneity levels were small-to-medium across all analyses (see Figs. S17–S24 in supplement materials for all time-points and sensitivity analyses).
Bias assessmentPotential publication biases were assessed visually with the help of funnel plots (Figs. S25–S27). The funnel plots do not suggest an asymmetry; however, the number of studies included was small, thereby increasing the likelihood of any deviation or adherence to the funnel shape being by chance. The funnel plots do suggest that studies are missing at the top and bottom for both significant and non-significant areas, which highlights a gap for studies involving larger sample sizes. The performed Egger’s tests were non-significant, thus indicating no bias due to small-study effects. However, funnel plots are influenced by multiple factors, of which publication bias is only one. Poor methodological quality and between-study heterogeneity could both influence the funnel plot in this review case. The conducted Galbraith plots suggest that two studies [19, 20] may have influenced the pooled effect size in the meta-analyses towards a greater reduction of child internalising symptoms (see Figs. S28–S32).
Meta-regressionsMeta-regressions were only performed for child and parent outcomes when sufficient studies were available. We included quality rating, type of control group and number of sessions as predictor variables, and mental health outcomes at first follow-up as the outcome. None of the meta-regressions suggested any significant effects for the included predictor variables. See Supplement materials 1 for results of meta-regression.
Synthesis of intervention experience and acceptability findingsDescription of studiesTwenty-two studies reported on families’ experiences with the interventions, the perceived benefits, and intervention acceptability. Ten of these studies, reporting on eight different interventions, described families’ experiences using qualitative methods. Together, these studies included 320 family members, of which 179 were parents/carers, 135 were children or young people, and 13 were former service users. Three papers included facilitators (n = 62) and/or referrers (n = 5). Four interventions targeted depression, one substance abuse, one anxiety, and three were open to multiple parental mental health illnesses. The majority of the interventions (62%; 5/8) were group interventions, providing 6–12 sessions, except for The Family Model providing only one session, and KidsTime being open-ended. Fourteen studies described acceptability in a quantitative manner, sharing experiences of at least 372 families (two studies did not provide sample size on family level), participating in 12 different interventions. Two studies (ID-n: 143, 173) provided attendance data, reporting attendance levels of at least 70% (of sessions/participants/active engagement), although there was no uniform way to assess attendance. One study evaluated an app-enhanced intervention (ID-n = 5), where engagement with the app was reported to be around 50% (of the days).
Description of themesWe derived three themes that describe families’ perceived benefits and outcomes of taking part and related intervention change mechanisms. In terms of intervention acceptability and families’ experiences of taking part, we summarised the evidence in four themes (Table 5).
Table 5 Themes, descriptions, and quotesTopic 1: Perceived benefits, outcomes, and change mechanismsFindings from the qualitative studies suggest that most families reported feeling positive about the outcomes of the interventions they had received and described it as a helpful experience. In some studies (ID-n: 2, 15, 214), participants described not noticing specific changes or improvements in response to the intervention (“To be honest no, I don’t think it made any great difference in the long run” parent, ID-n: 2). Two studies assessed whether any harm was experienced by participating families, and nothing was reported.
Theme 1: Learning, understanding, and skill development. Studies commonly highlighted that interventions enhanced participants’ levels of understanding, knowledge, and skills. Families reported that receiving practical information (e.g., who to call when, how to structure a day) and psychoeducation (general and specific to PMI) not only increased their knowledge and mental health literacy but also helped them feel more confident (ID-n: 2, 10, 16, 59, 79, 91, and 214). Sharing experiences with other families and family members contributed to a better understanding of different perspectives (e.g., the impact of PMI on children and partner) and supported mutual learning sometimes by exchanging practical advice (ID-n: 10, 79, 214). Some studies described families’ mentioning intervention-specific outcomes, such as children reporting that they had learned new coping and problem-solving skills which helped them with reducing stress, anxiety and worries (ID-n: 16, 91). Many interventions aimed to improve parenting skills, by providing feedback, support, and advice around parenting. Parents in these interventions primarily reported to have benefited from the support and feeling more confident as parents (ID-n: 2, 16, 206). Some parents wished for more ongoing support as their children are getting older (ID-n: 2). Changes in parenting as reported by parents were not always noticed or reported by their participating children (ID-n:2).
Theme 2: Enhanced family environments and relationships. Many families reported that interventions had created more warmth in their families and increased bonding between family members, including parent–child, couple, and sibling relationships. Exercises that encouraged sharing of experiences and perspective-taking between family members were described as bringing family members closer together by making sure everyone’s voice is heard and validating different experiences. Interventions that involved activities for the whole family (e.g., fun activities, talking about strengths) were perceived to increase families’ confidence and trust. Most families described that they enjoyed spending time together as part of the intervention. For some families, this naturally led to more engagement in family activities outside of the programme. Parents also noted that building a “united front” helped them be better parents. Some interventions were described as contributing to healthier family dynamics, by helping with the shift in roles and responsibilities (e.g., children having less responsibility).
Many families described being more able to talk about PMI in their family, and that interventions had helped parents by finding age-appropriate words to talk about mental illness and families by developing a shared language for these conversions. However, talking about PMI as part of the intervention was experienced as challenging by some families (ID 206). Occasionally, families reported that they did not notice any changes in the way they spoke about PMI in comparison to prior intervention. Families also noticed general improvements in communication within the family and explained that they had learned to listen better and respect each other, which in turn led to fewer conflicts, better problem-solving, and increased understanding and support for each other (ID 10, 79, 91, 206).
Theme 3: Normalisation and like-mindedness. Meeting other families and peers in interventions and having the opportunity to share experiences was associated with reduced feelings of stigma, guilt, and shame. Families explained that hearing similar stories helped them feel more normal (ID: 10, 16, 59, 79, 91, 206, 213, and 214). Many young people and adults also shared that they benefited from making new friends and meeting families who lived in similar circumstances, which made them feel less alone. It also helped them feel more comfortable and safer around them, as opposed to friends and peers that they had elsewhere, for example at school (ID-n: 10, 59, 79, 214). These benefits were primarily reported in interventions with peer or group components.
Topic 2: Intervention acceptability and families’ experiences of taking partStudies that assessed acceptability and satisfaction rates via questionnaires mostly reported high satisfaction scores (ID-n: 5, 62, 91, 118, 123, 132, 135, 201, 179, and 214). When questionnaires were specific enough, family members tended to rate the support and information received by facilitators the highest, and homework assignments or exercises somewhat lower on satisfaction scales. The only exception was Family Strengths (ID-n = 91), where participants especially appreciated the family exercises (e.g., family fun time). The five themes below summarise the qualitative findings from ten studies.
Theme 4: Initial engagement. Studies that explored families’ reasons, motivation, and expectations to take part described that some families had been unclear about the purpose of the intervention, but that most parents had hoped to support their children better. Due to the limited understanding, families could not always provide clear reasons for attending but explained in many cases that the intervention was the only support offered to them. The uncertainty about the intervention and lack of information about what it would entail resulted in families feeling initial apprehensions about taking part. Many participants reported feeling anxious and nervous at the beginning of the intervention but that this had eased over time.
Theme 5: Role of facilitators. Facilitators were often mentioned as important drivers for engaging families in and for the acceptability of the intervention. Almost all studies talked about the facilitators being welcoming, non-judgemental, and following a strength-based approach. Several studies provided positive feedback on the flexibility of facilitators and their ability to adapt to individual circumstances. For children, the fun and welcoming atmosphere created by facilitators was important for satisfaction and engagement with the intervention. In one study (ID-10), parents shared their negative experiences with the facilitating team and described initial meetings and assessments as invasive and not family-centred. Parents in the same study reported that facilitators had been overinvolved, calling children’s schools and putting too much pressure on participating parents.
Theme 6: Intervention content. Families’ satisfaction with the content of interventions varied. Most families gave positive feedback about intervention content and reported that it had contributed to the perceived benefits (e.g., learning) and positive changes. Families also provided suggestions on how interventions could be further improved. One study reported that the impact of PMI had not been addressed enough, while some studies indicated that (Young Smiles, Family Strengths, and Family Talk) that parents had found that the intervention had focused too narrowly on PMI and/or the impact it had on the children, which occasionally made the affected parent feel uncomfortable and that they were the “cause” of the problem or the one to blame. Some families also explained that they wished for more wider issues and concerns to be addressed as their and their children’s mental health and well-being were impacted by other factors unrelated to PMI (e.g., housing, and physical health problems). Interventions with group components were often criticised as not being suitable or engaging enough for different age groups, specifically psychoeducation and activities, and inaccessible for individuals with disabilities (ID-n: 59, 214). Families who took part in interventions that included playful and/or creative activities experienced these as helpful in terms of practising and exploring new skills, but also described them as fun and enjoyable which had helped them feel more positive generally and also by giving them time away from home (“Home was sad, Kidstime was fun. That’s what I looked forward to. I looked forward to having fun, you know being a child. But at home you have to be an adult, look after yourself, look after mum”—child ID-n: 59).
Theme 7: Intervention format, structure, and logistics. As mentioned above, interventions with a group format were generally associated with many positive experiences by families, including meeting other families, sharing experiences, feeling less socially isolated, and learning from others. In some studies, parents reported that the group size had been too big, which had made them feel stressed and in some cases also led to discontinuation with the programme. The group format was also described as being anxiety and shame provoking when having to share personal experiences with new people. At times they could also feel overwhelming and unsafe. In one study, parents shared their frustration about in-active participants and participants behaving unprofessionally (ID-10). Participants repeatedly emphasised the importance of having sufficient time to “settle in” to feel safe and build trust with other participants. Families also described that these concerns were more easily overcome in groups that were informal and felt non-judgemental and welcoming.
Most interventions followed a regular structure with weekly or biweekly meetings. Families reported that they appreciated a regular structure and manualized approach, but occasionally families described having to attend weekly meetings and doing homework exercises could be challenging and tiring. They wished for more flexibility to meet families’ needs. Most of the interventions evaluated were closed-ended interventions, with a fixed number of sessions. Many families shared that they needed more sessions to sustain and implement the achieved changes and that they hoped for more continuous support, as in many cases no other support was available once this specific intervention had finished. Some parents explained that they wanted more support as their children got older and some families simply wished to keep in touch with other group members to maintain their new social support network.
Families considered the environment where the intervention took place as important and commented on certain settings and locations pointing out that some felt more welcoming (e.g., community centre) than others (e.g., clinic, small rooms). Occasionally, it was reported that locations were hard to reach for families which could impact attendance and engagement in the programme.
Interventions providing mainly family sessions were praised for their whole-family approach, whereas participants from other interventions requested to include more family members (ID 16) or to have more whole-family sessions rather than separate parent and child sessions only. In one study (ID91), parents wished for more adult time to work on their marital relationship. For young people, the data suggested that adolescents preferred adolescent-only over the parent–child sessions, based on higher satisfaction and alliance ratings (ID-n = 62) and young people explaining that the child-only sessions provided space where they could be autonomous from their parents and which provided some respite (ID-n: 10).
Comments (0)