
Remember me
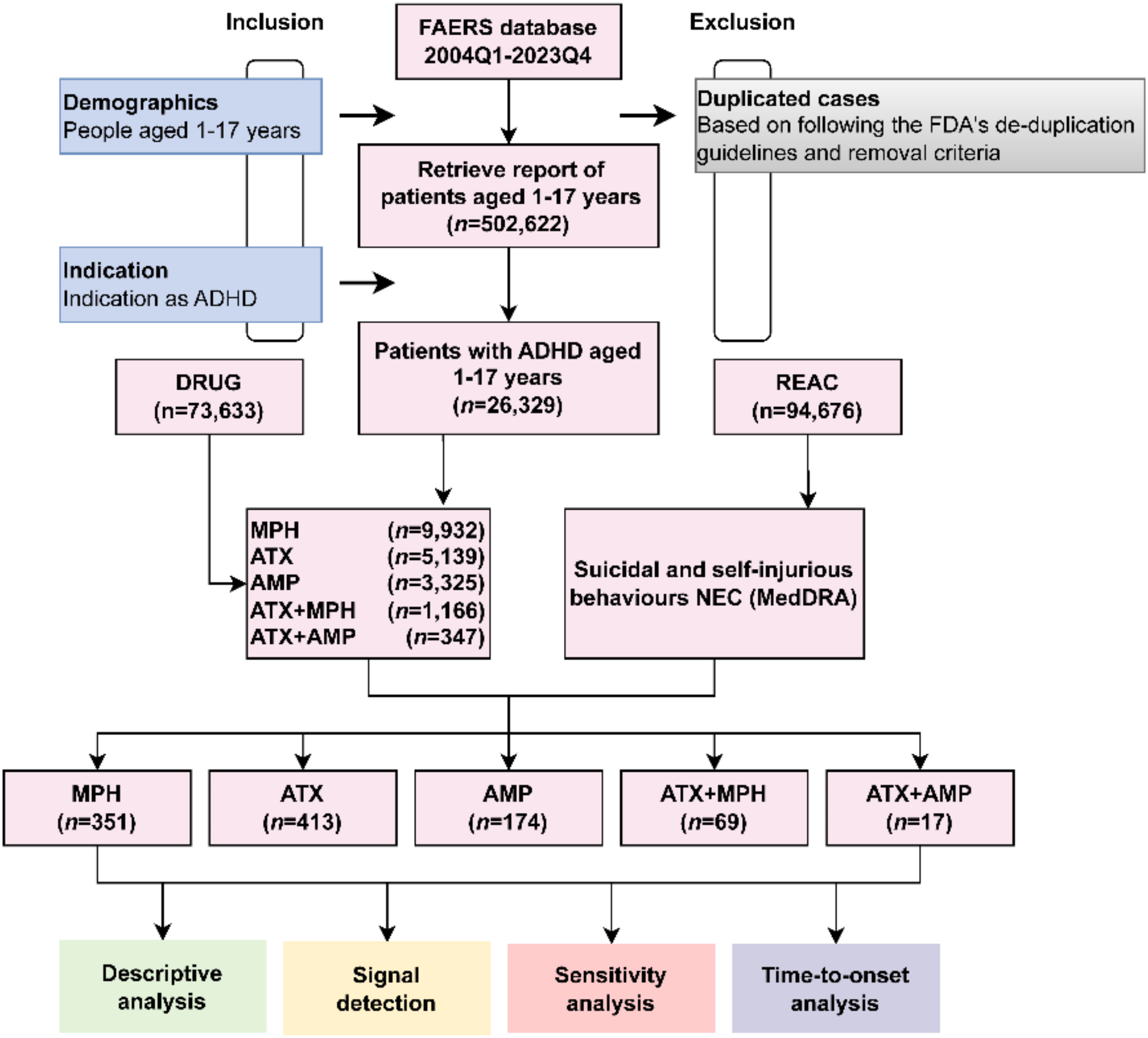
The study selection process is illustrated in Fig. 1, following PRISMA guidelines [57]. The initial screen yielded 9031 results. After duplicates were removed, 5852 articles were initially screened according to eligibility criteria based on title and abstract, where 5605 records were excluded. Five additional studies were identified through reference screening. As 23 studies could not be retrieved, primarily due to being a conference abstract without a corresponding full-text article, 229 full-text articles were assessed for eligibility, and 188 were excluded. As seen in Fig. 1, the primary reasons for exclusion at full-text screening includes: articles being review papers (n = 21); failing to explore factors that influence ADHD diagnosis (n = 40); only reporting on prevalence rates of ADHD in different groups without addressing whether or how these group characteristics relate to the ADHD diagnostic pathway (n = 31); and only investigating community, organisational, systemic and societal level factors (n = 32). For example, Efron et al. [61] investigated predictors of professional service use in children with ADHD, but the factors affecting care did not specifically relate to the ADHD diagnostic process. Another example is Collins et al. [62], who used a population-based survey to examine ethnic disparities in parent-reported diagnosis of ADHD, but its primary aim was to examine trends of ADHD prevalence rates, without addressing how these disparities relate to the ADHD diagnostic process.
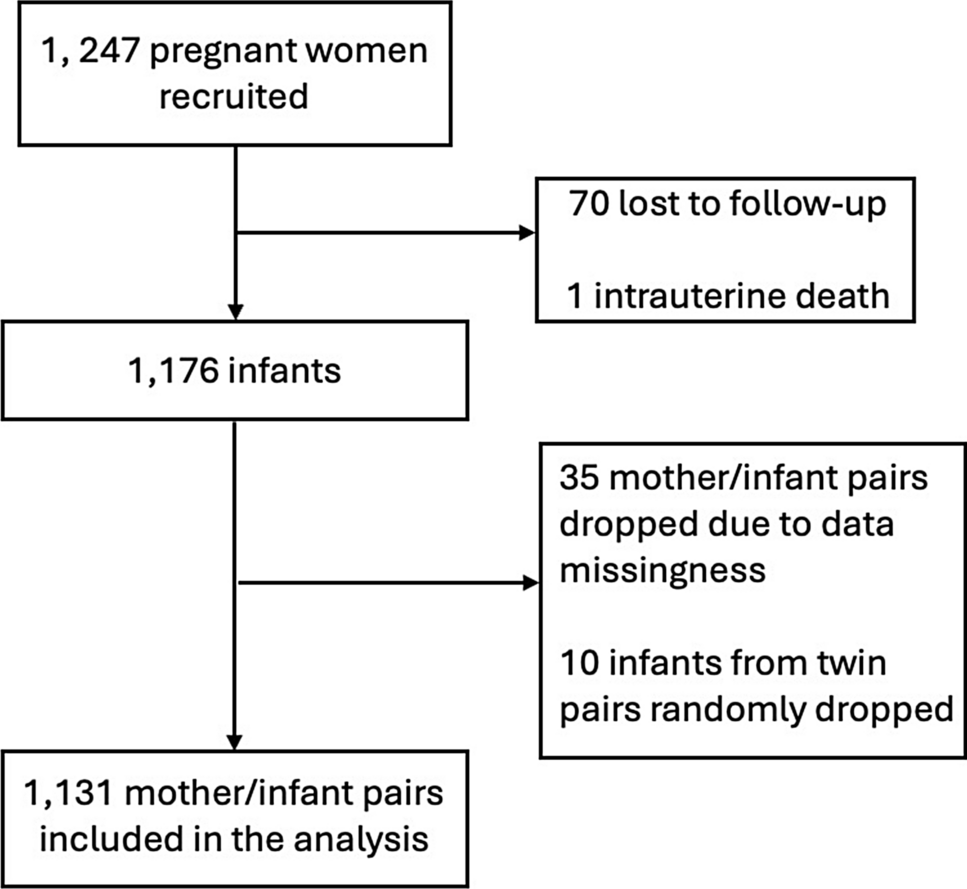
Fig. 1
PRISMA flow diagram illustrating the selection process of the systematic review
Forty-one studies met eligibility criteria and are summarised in Table 1 and in the Supplementary Materials 2. Most studies (26/41) reported the impact of the child-level factors on the overall presence of an ADHD diagnosis [33, 35, 42, 63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85], while a smaller number reported on the specific steps within the ADHD diagnostic process (7/41) [86,87,88,89,90,91,92], the age of ADHD diagnosis (4/41) [93,94,95,96], or delays within specific steps in the ADHD diagnostic process (4/41) [97,98,99,100]. Of the 41 included studies, 17 were from the USA, five from the UK, three from Sweden, two from Germany, two from Italy, two from Taiwan, and the remaining were from Bosnia and Herzegovina, Brazil, Canada, Denmark, Finland, France, India, Ireland, Japan, and Norway. A number of different methodologies were used by included studies, but all were quantitative. None of the included studies reported any conflicts of interest. Most studies were published in peer-reviewed journals, except for three unpublished dissertations [92, 94, 96].
Table 1 Included studies and participant characteristicsCritical appraisals of all included studies can be found in the Supplementary Materials 3. The quality appraisal revealed that the highest proportion of included papers (34; 82.9%) received low ratings for the domains of participant selection and measurement of child-level factors. This is due to the high number of population-based cohort studies and large community-based samples, which have a relatively low risk of selection bias. For child-level factors, much of the data relied on trustworthy sources such as medical records, and/or used well-validated measures as the Strengths and Difficulties questionnaire (SDQ) [101]. Conversely, a significant proportion of studies (12; 29.3%) had a high risk of bias caused by inadequate blinding of outcome assessments. Moreover, 12 studies (29.3%) inadequately considered potential confounds, a concerning observation given that the receipt and timing of ADHD diagnosis depends on a complex interplay between child and contextual factors. Additionally, a significant number of studies (20; 48.8%) did not report their approach to handling missing data.
Overall, 16 child-level factors were identified as influencing the diagnosis of ADHD in children and adolescents. The clinical factors include ADHD subtype, comorbid mental disorders, behavior problems, internalizing symptoms, ADHD symptom severity, impairment, social and cognitive functioning, and general health; whereas the sociodemographic factors included age, gender, relative age, race/ethnicity, SES, insurance status, urban or rural residence and family structure.
SubtypeFour papers examined the impact of ADHD subtypes on the receipt or timing of an ADHD diagnosis [33, 96, 97, 99]. In a nationally-representative sample of US children [33], children who met DSM-IV criteria for ADHD-C were approximately 10% more likely to have been previously diagnosed with ADHD than children who met criteria for ADHD-HI only. A further 10% of children who met criteria for ADHD-C were more likely to have been previously diagnosed with ADHD compared to those who met criteria for ADHD-I only. However, these differences were not statistically significant.
Regarding age at diagnosis, in a student sample from rural northeast Georgia, children with ADHD-C were previously identified and diagnosed by a psychologist or psychiatrist at a significantly younger age than their ADHD-I counterparts [96]. Children with ADHD-C demonstrated the fastest access to specialist services for evaluation from the onset of symptoms, followed by ADHD-HI, while children with ADHD-I experienced the most substantial delay in referral to a specialist [97]. Children with ADHD-I had a median delay of 6 years, which was twice as long as the delay observed in ADHD-C children. However, another study showed that once in contact with professionals, there were no significant differences in the time required for a formal diagnosis among children with varying ADHD subtypes [99]. Overall, findings suggest that children with the ADHD-I subtype may experience the most delayed diagnosis, and that the ADHD subtype may exert a more pronounced influence on the diagnostic steps preceding specialist services, rather than on the diagnostic process once the child is in contact with specialist services.
Mental health comorbiditiesSix papers examined the effects of diagnoses of comorbid mental disorders, irrespective of the exact nature of these disorders, on ADHD diagnosis [84, 89, 90, 93, 97, 98]. These studies grouped various mental health conditions together as one factor. For instance, Arya et al. [97] combined ODD, CD, and substance use, whereas Sikov et al. [84] combined anxiety, depression, disruptive behavior disorders, learning and developmental disorders, and mood disorders together as one group. Findings regarding the impact and directionality of mental health comorbidities on the identification of ADHD were inconsistent. Sikov et al. [84] suggested that the presence of comorbid disorders increased the likelihood of receiving an ICD-10 ADHD code in primary care health records. However, while a population-representative sample from the 2004 British survey indicated that the presence of comorbid mental disorders increased parental recognition, professional contact, and referral [89] these factors were not significant predictors in the 1999 survey conducted five years earlier [90]. As both studies employed the same study design and methodology, the different results may be attributed to changes in context between the study years.
Regarding the timing of diagnosis, two studies suggested that the presence of comorbid disorders may reduce the duration of the diagnostic process, showing that children with comorbid conditions had a decreased delay in help-seeking and contacting specialist services in a newly registered outpatient sample [97], and a younger age at recorded clinical ADHD diagnosis in primary care health records [93]. However, Bonati et al. [98] found that comorbidity did not significantly affect the time taken to receive a diagnostic evaluation for children who had already enrolled into regional specialised ADHD referral centres.
These studies all originated from diverse countries, encompassing the USA [84, 93], UK [89, 90], Italy [98] and India [97]. There was also study variation in the types of comorbid diagnoses examined. For instance, Arya et al. [97] focused on ODD, CD, and substance use, whereas Sikov et al. [84] included a broader range of diagnoses, such as anxiety, depression, disruptive behavior disorders, autism spectrum and developmental disorders, and mood disorders. Given these disparities, and the heterogeneity in findings, a definitive conclusion cannot be drawn.
Disruptive behavior problemsDisruptive behavior problems, including conduct problems, aggression, and ODD/CD symptoms, were examined in eight studies [77, 80, 86, 91, 92, 94, 99, 100]. In these studies, disruptive behavior was assessed via parent-report [80, 99, 100], teacher-report [77, 86, 92], or by both informants [91, 94] using well-established instruments or semi-structured interviews.
Among these papers, three studies indicated that disruptive behavior facilitated the diagnosis of ADHD. Conduct problems and aggression were linked to an increased likelihood of an ADHD diagnosis [77], recognition and referral by teachers [92], and PCPs [91], likely due to enhanced impairment and problem recognition. The potential confounding variables adjusted by these studies included age, race/ethnicity, SES, and academic achievement, except for Staniszewski [92], which did not include any adjusted models. However, two studies did not find a relationship between disruptive behavior and ADHD diagnosis. Barry et al. [86] found that disruptive behavior had no significant effect on the likelihood of parental recognition and acceptance of the recommendation for an ADHD referral. O’Connor and McNicholas [80] also did not find a significant difference between the behavior problems of children diagnosed with ADHD and those exhibiting ADHD symptoms at age nine who were not diagnosed at the time, despite diagnosed 9-year-olds tending to score higher on behavior problems than their undiagnosed peers. The authors controlled for additional potential confounding variables, such as ADHD symptoms, cognitive ability, general health and service engagement, which may have moderated the relationship between behavior problems and ADHD diagnosis.
Three studies examined whether disruptive behavior problems affected the timing of ADHD diagnosis, all with differing findings. Hlavaty [
Comments (0)