Bleeding Jejunal Diverticula: Always a Timely Reminder
Patients with jejunal diverticulosis (JD) disease are largely asymptomatic and often go undiagnosed. The true incidence is therefore unknown. The widely quoted incidence is between 0.06 and 1.5% [1]. Acquired JDs are pulsion pseudo-diverticula that arise consistently on the mesenteric side of the bowel; this feature may contribute to difficulty in their identification in the mesenteric fat. JDs develop at the point of the vasa recta vascular penetration of the circular muscular layer, unlike diverticula in the colon which typically develop in parallel rows between the taenia coli. Aetiologically, like colonic diverticulosis, chronic raised intraluminal pressure is implicated on the basis of small bowel dyskinesia and dis-coordinate peristalsis [2]. Usually, small bowel diverticula are more common and larger (up to 10 cm in size) in the proximal jejunum (presumably due to the larger vasa recta of the jejunum) and decrease in size and number toward the ileum [3].
Even though the clinical awareness of JD may be triggered by the triad of abdominal pain, anaemia and segmental bowel dilatation at epigastrium or left upper abdomen, establishing the diagnosis and localisation of JD bleeding may be elusive due to the relative inaccessibility of the jejunum to standard endoscopic techniques [4]. In the largest series (68 patients) to date reporting on a two-decade experience with JD, CT scan was the most commonly utilised diagnostic tool for JD bleeding, followed by enteroscopy, angiography, enteroclysis and surgery. The diagnostic accuracy for JD bleeding was 35% for CT scan, 87.18% for enteroscopy, 14.29% angiography, 88.89% for enteroclysis and 100% for surgery [5].
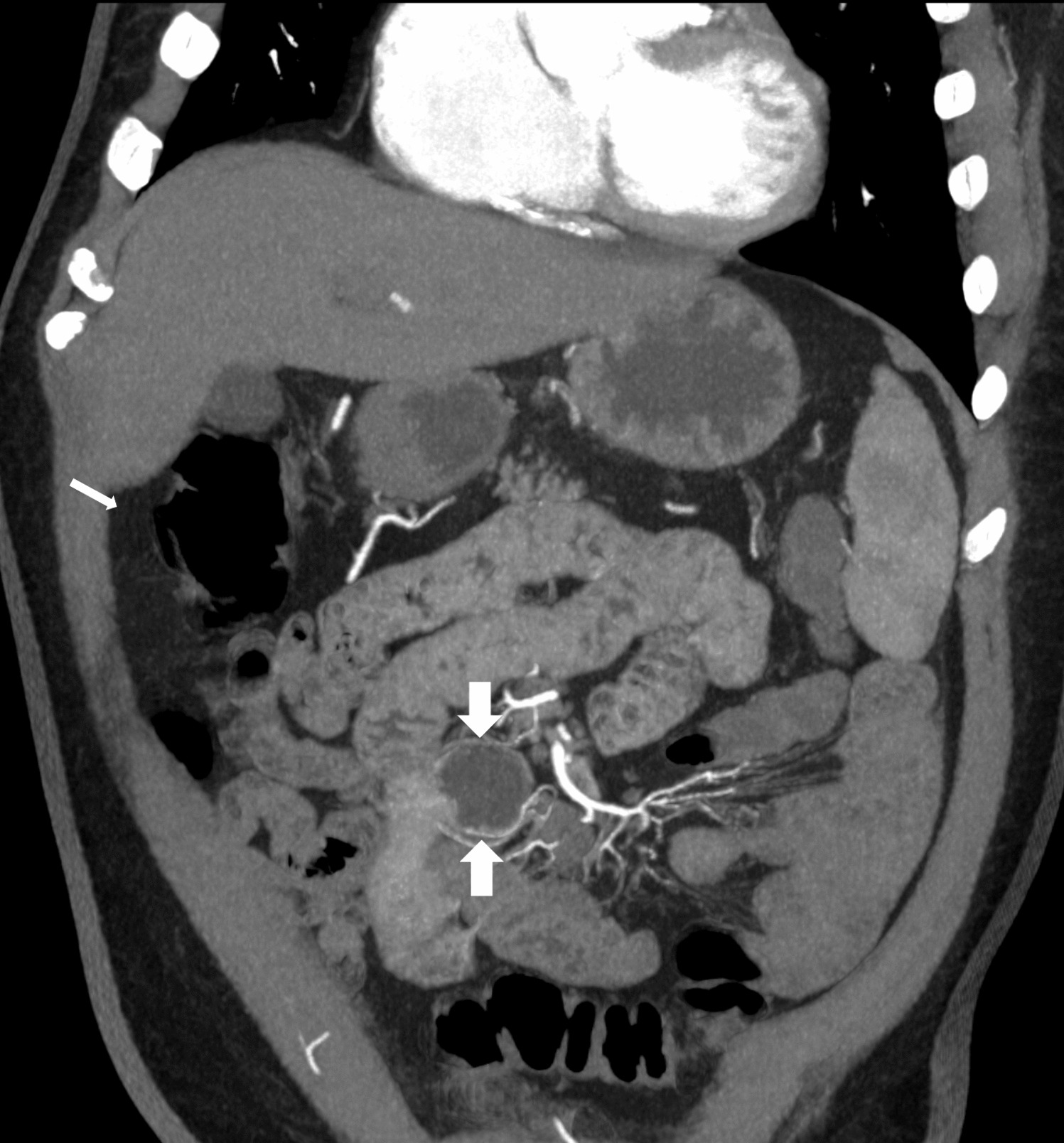
A reasonable approach is to perform upper and lower gastrointestinal endoscopy in all cases presenting with lower gastrointestinal bleeding. With a negative or inconclusive endoscopy, our preferred diagnostic approach is abdominal MDCT scan to provide a roadmap for further treatment; this provides the detection of active bleeding as well as demonstration of morphologic changes, such as intestinal tumours. If numerous JDs are encountered intra-operatively, the identification of the incriminating bleeding diverticula can be confirmed by employing an on-table push enteroscopy, single-balloon enteroscopy, double-balloon enteroscopy or spiral enteroscopy.








Comments (0)