This was the first survey among HCPs in Japan to evaluate the effectiveness of aRMM material. The results of this survey revealed that pharmacists explained how to take IXA to patients and that the aRMM material was utilized at the time of the explanation. As the environment for evaluating the effectiveness of aRMMs in Japan is not well established and the number of previous surveys is limited, this study may serve as a valuable reference for how such surveys should be conducted in Japan in the future.
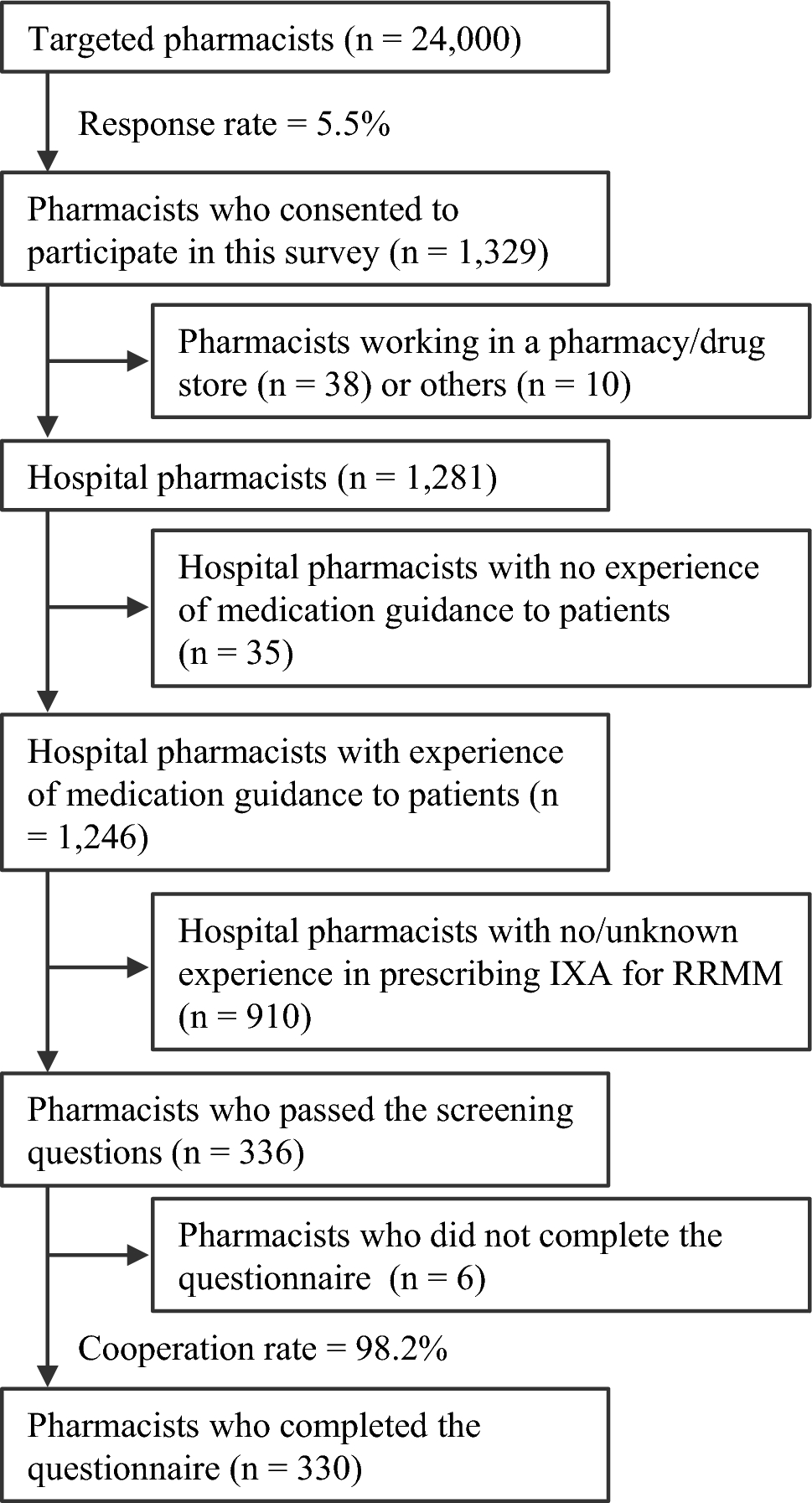
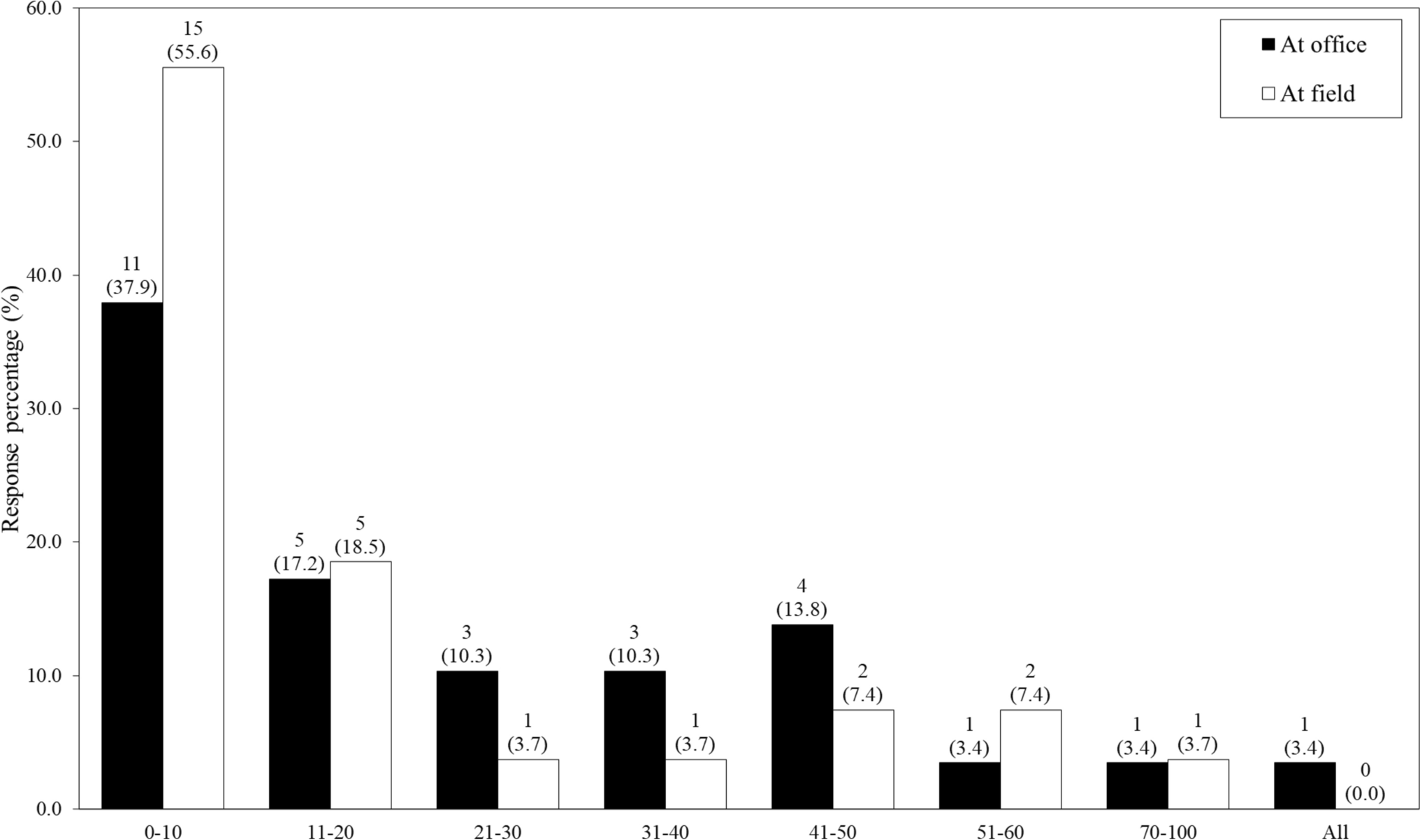
Among the participants in this survey, no pharmacists belonged to clinics, and approximately half of them worked in hospitals with ≥500 beds. This indicates that our analysis population was an appropriate target for this survey, as IXA is dispensed mainly at designated cancer care hospitals, many of which are regional core hospitals or larger [13]. In addition, more than three-quarters of the respondents had ≥ 10 years of experience as pharmacists. This is likely due to this panel including a large number of highly specialized HCPs. A similar trend was observed in a survey conducted in Japan among other healthcare professional panels [14, 15].
Most pharmacists explained how to take IXA to their patients. However, the proportion of pharmacists with experience in using the aRMM material at the time of explanation was approximately 30%. This result is related to the fact that 187 of the 307 pharmacists who explained the contents of the aRMM material responded that they had never obtained the aRMM material. This may be because there are multiple materials containing instructions on how to take IXA. The results of Q5 (see Supplementary Table 4 in the ESM) suggested that comprehensive materials, including information on adverse events, were utilized more frequently than materials focusing on the dosing schedule of IXA. However, of those who responded that they “had obtained the aRMM material” and “explained how to take IXA to patients,” approximately 70% answered that they had used the aRMM material, suggesting that the aRMM material was being used.
Approximately 40% of respondents answered that they had obtained the aRMM material. Compared with the overall results (37.6%), a higher proportion of pharmacists working in specialized medical institutions for cancer treatment (100.0%), pharmacists specialized/licensed in cancer treatment (50.0%–71.4%), and pharmacists who fully understood the RMP for IXA (81.3%) responded that they had obtained the aRMM material. These results suggest that institutions and individuals expertized in cancer treatment obtained aRMMs more frequently. In addition, they understood the importance of explaining how to administer IXA to patients.
Globally, several challenges have been identified in the evaluation of the effectiveness of aRMMs, including difficulties in choosing feasible indicators (process and outcome indicators), burden on the healthcare system, barriers to patient and HCP access, challenges in setting thresholds for effectiveness, timing and frequency of conducting the studies, and choice of appropriate study designs and data sources [12]. Of these, the major challenges in this survey were the inability to consider outcome indicators due to feasibility and the fact that the pre-determined thresholds for effectiveness could not be set due to the limited availability of reference information.
We also identified several specific challenges in Japan regarding the effectiveness evaluation. First, measuring the effectiveness of a single piece of educational material is challenging. In Japan, the proportion of newly approved products with aRMMs is higher than in Europe and the US [16]. In addition, these materials have been used for a long time. Furthermore, multiple materials for patients/HCPs other than those developed as aRMMs commonly contain similar information. Consequently, patients and HCPs are routinely informed through numerous media sources, which makes it difficult to measure the effectiveness of a specific material alone. To overcome this, the primary endpoint of our survey was set to whether the ‘contents’ of the aRMM material are explained. Second, a unique feature of Japan is that many materials prepared as aRMMs are not intended to minimize specific risks but rather provide a comprehensive overview of the product covering various risks. Considering the risk-management cycle of medicinal products and the objective of aRMMs, defining educational materials only for specific risks as aRMMs is considered more effective. These challenges regarding the effectiveness evaluation of aRMMs warrant further discussion in light of future appropriate regulations and cases evaluated for aRMM in Japan.
Some limitations exist in interpreting the results of this survey. The first is due to selection bias. As this survey was conducted online only and the population actively participating in the survey may have different characteristics, such as higher motivation to obtain information, the analysis set may not be completely representative of the population. The second limitation is social desirability bias, in which pharmacists tend to give socially desirable/expected responses instead of reflecting on their current knowledge or behavior. This relates especially to the binary response questions, such as the questions on whether pharmacists understand how to take IXA (Q1) and whether they explain how to take IXA to patients (Q3), which may have been affected by this bias, resulting in a potential overestimation of the proportion of ‘Yes’ answers for these questions. Lastly, since this survey was self-reported and the time of obtaining the material and prescribing IXA depended on each respondent, recall bias may have occurred. Additionally, pharmacists are assumed to obtain many materials daily, which may cause confusion. However, we attempted to minimize confusion in the survey by presenting on-screen photographs of the materials during the questionnaire.




Comments (0)