
Remember me



Rheumatologic diseases are notably heterogeneous due to underlying immune-mediated metabolic or mechanical processes. This can lead to joint destruction such as in rheumatoid arthritis (RA), or can affect various organs, as seen in systemic lupus erythematosus (SLE) and other collagen vascular diseases. Additional factors, such as depression, fibromyalgia, calcifications, or osteoarthritis, often play a role, adding to pain and inflammation stimuli [1]. Diverse patho-mechanisms operate at the cellular level, and even within the same disease, they can vary [2]. For example, RA can exhibit a lymphocytic proliferation on a T- and B-cell level with an invasive reaction of fibroblasts, or alternatively, pauci-cellular macrocytic inflammatory reactions or fibrosis [3]. In return, each pathotype reacts differently to targeted disease-modifying therapies [4]. This diversity is reflected at the cytokine level, with varying responses to cytokine blockade (e.g., tumor necrosis factor [TNF], interleukin [IL]-6, IL-17, or IL-23) or cell depletion (CD20) [5]. Despite an ever-expanding arsenal of medications, in most clinical trials, two-thirds of rheumatology patients still do not achieve complete remission [6]. It is crucial to note that assessing disease activity and defining remission in rheumatology is not straightforward. RA alone has a plethora of indicators, such as DAS28, ACR50, Clinical disease activity index (CDAI), EULAR/ACR remission, etc. [7]. Additionally, patients have diverse priorities, with improvements in fatigue or morning stiffness being major concerns, although their measurement remains subjective. In this sense, we mostly follow the treatment recommendations of EULAR/ACR, but this is a systematic, but so far not at all personalized, approach to treating RA or other rheumatic diseases [8]. Meeting these needs requires time, which is unfortunately insufficient due to a shortage of rheumatologists [9]. Other clinical needs include better interdisciplinary coordination of treatment, for example for psoriatic arthritis or arthritis in chronic inflammatory bowel disease. For various reasons, we still think and act in silos, which does not necessarily benefit patients and health care professionals. Finally, there are several rheumatic diseases, such as osteoarthritis of the hand or fibromyalgia, for which no satisfactory drug treatment is yet available [10].
1.2 Digital TransformationThe COVID-19 pandemic has ushered in the era of telemonitoring. In the United States, for instance, telemonitoring of patient-reported outcomes is financially rewarded as a quality assurance measure [11]. Increasingly, patients collect data through apps or wearables, some of which are compatible with electronic medical records (EMRs) and are stored there [12]. This integration of structured and unstructured clinical data with radiological, laboratory, and immunological data helps create a more comprehensive and personalized profile of rheumatology patients, facilitating better prognosis [13]. EMR providers have recognized this trend and are increasingly involved in developing algorithms that can be integrated directly into EMRs as clinical decision support tools [14]. All of these advancements lay the foundation for a more patient-centered and decentralized approach to medicine, addressing the shortage of rheumatologists or radiologists. Alongside personalization, automation is a fundamental trend, allowing the automation of simple processes such as prescription refills for stable cases or dynamic scheduling through digital tools. Communication with patients can also involve chatbots, deep learning algorithms or advanced language models like ChatGPT4 to handle certain needs, and potentially appointment rescheduling or insurance inquiries [15]. Finally, the internet of things (IOT) and improving sensor and camera technology permit connected medicine with wearables or motion capturing and measurement of mobility as functional biomarkers [16].
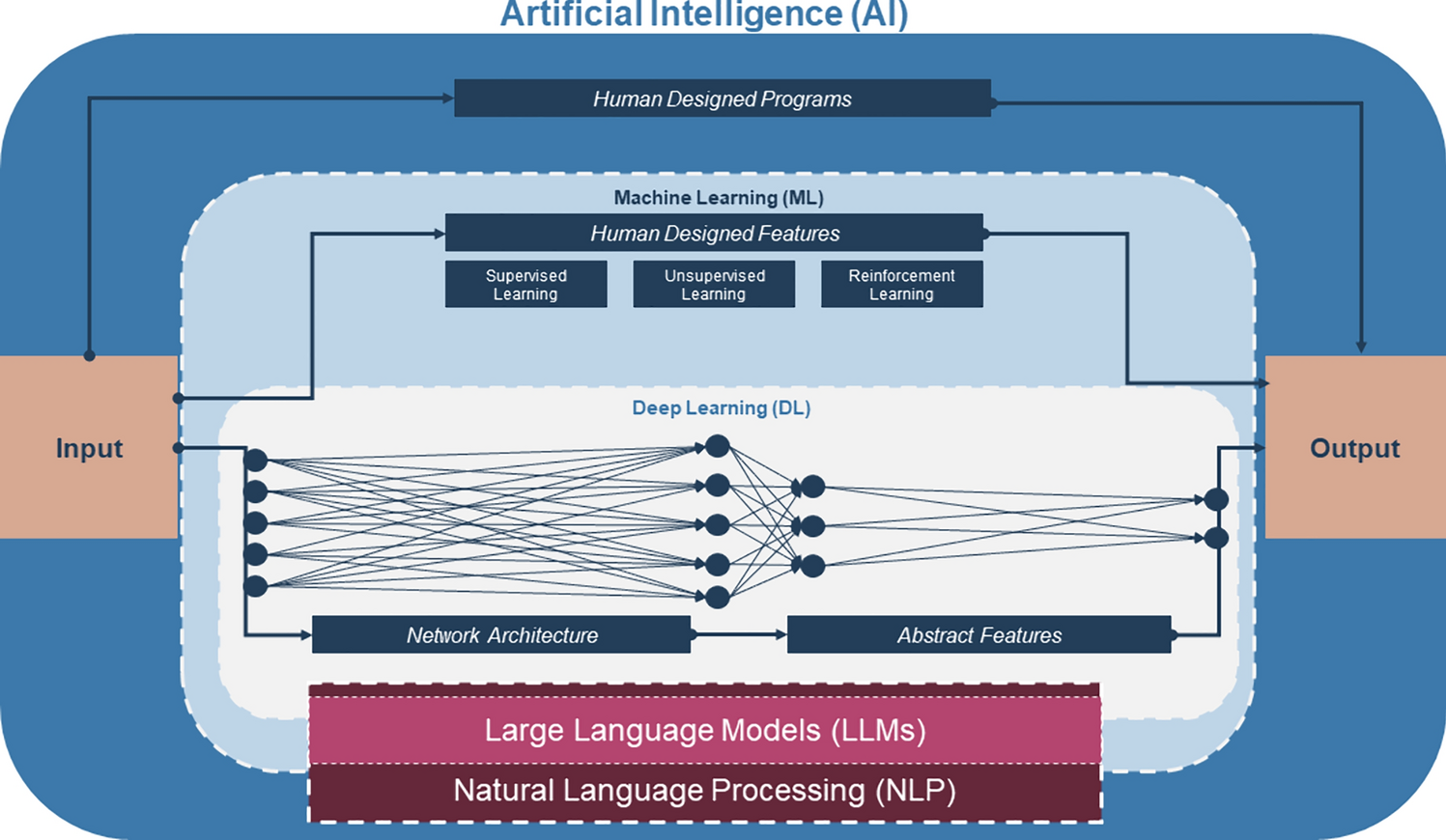
1.3 Machine LearningWe are amassing an overwhelming amount of data from our patients, beyond human capacity to manage. This is evident in the expanding array of digital clinical outcome assessments, digital biomarkers, or -omics data, which are now being collected through self-sampling from home along with different imaging modalities that increasingly include photos and videos by patients and doctors [17]. Machine learning allows us to build models to learn from previous data in order to deliver predictions or image recognition [18]. Most of the time, supervised learning models are applied, meaning that the model obtains labeled data (e.g. x-rays with information on erosions, osteophytes etc.). After definition of the output variable of the algorithm, datasets are then divided into a training set (typically 80%) and a test set (20%). The output variable usually is defined as a classification task, such as remission at next visit or a radiographic finding yes/no. In the field of osteoarthritis, this is the case in 90% of the currently published studies (Fig. 1) [19]. Each model should be validated in an independent dataset that is representative for the population where it is applied. Unsupervised learning, that is, algorithms based on unlabeled data, is less frequently applied than supervised learning. Unsupervised learning is used for clustering such as defining disease phenotypes or finding patient outliers in EMRs [20]. Finally, reinforcement learning is the third pillar of machine learning. Reinforcement learning is based on a reward function, or in other words on trial and error. Here, the algorithm is allowed to make new decisions, but has to learn from mistakes (and successful decisions) [21]. Quite advanced in diabetes mellitus, reinforcement learning is not yet applied in the field of rheumatology [21]. In diabetes, it can be applied in a closed system with a simple biomarker (blood glucose) and a simple intervention (insulin injection). A scenario where reinforcement learning could be applied in rheumatology could be in relatively simple tasks, such as adjusting cortisone doses under strict rules in terms of dose, frequency, etc. Based on the clinical or laboratory response, the model, here also called ‘agent’, would perform or propose an action that then again will be evaluated by the reward function.
Fig. 1
Overview of domains in artificial intelligence. Supervised machine learning is by far the most widely used, mostly through labelled clinical data such as X-ray images. This is followed by unsupervised learning with unlabeled data, e.g. electronic medical records. Reinforcement learning allows algorithms to make their own decisions and correct them. Complex language models such as ChatGPT use a combination of supervised, unsupervised, and reinforcement learning
Transfer learning is another machine learning method where a model already developed for a task is reused in another task. Transfer learning is a popular approach in deep learning, as it enables the training of deep neural networks with less data compared with having to create a model from scratch.
In general, the more data that is available to train a machine learning model, the better. However, it's important to recognize that more data doesn't necessarily equate to better data. Clinical judgment and data pre-selection remain crucial, and we must correctly assess data quality and validate algorithm applicability across different patient groups. Currently, over 500 algorithms are FDA approved, with the majority focused on imaging in radiology, cardiology and pathology [22]. Table 1 overviews the different domains of AI.
Table 1 Domains of artificial intelligence (AI)This article begins by discussing imaging, where AI has made significant progress in clinical applications, and then delve into clinical prediction and digital biomarkers. Finally, we will discuss the integration of these applications into the clinical workflow and in clinical trials.
Comments (0)