
Remember me
Dear Editor,
Flagellate erythema is a distinctive type of cutaneous eruption characterised by the sudden onset of parallel, linear or curvilinear plaques, typically on the trunk, resembling whiplash marks. Originally identified as related to bleomycin toxicity,1 it can also be associated with the consumption of undercooked shiitake mushrooms and less commonly with rheumatological diseases and various chemotherapy drugs.2 We report a rare case of flagellate erythema associated with idiopathic dermatomyositis.
A 43-year-old man treated with tenofovir for hepatitis B and liver cirrhosis presented to our hospital with severe pruritic red-to-purple parallel streaks and acute proximal muscle weakness that began a month earlier. He reported owning a cat and using vegetable cat litter but denied consumption of mushrooms or use of bleomycin.
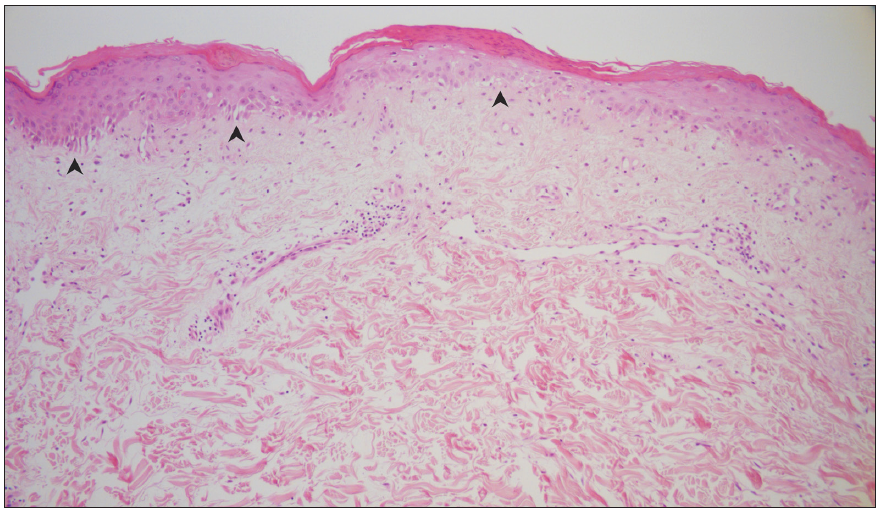
Physical examination revealed persistent erythematous parallel streaks on the trunk, accompanied by the shawl sign, the V sign and confluent patches on the buttocks [Figures 1a and 1b]. In addition, Holster sign [Figure 1c] and Gottron’s papules were present, along with a heliotrope rash and periorbital oedema. Serum biochemistry revealed elevated levels of creatine kinase (8108 IU/L), aspartate aminotransferase (344 IU/L), alanine aminotransferase (151 IU/L) and lactate dehydrogenase (863 IU/L). Antinuclear antibody was weakly positive, whereas other autoantibodies, including the anti-Jo-1 antibody, were negative. A skin biopsy of a violaceous parallel streak from the lower back showed interface dermatitis and superficial dermal perivascular lymphoplasmacytic infiltration [Figures 2a and 2b]. T2-weighted fat-suppressed magnetic resonance imaging of the hips revealed symmetrical bilateral muscle hyperintensities of the buttocks and thighs. Muscle biopsy revealed muscle fibre necrosis with regeneration and minimal inflammation. These findings were consistent with those for dermatomyositis. Additional studies, including colonoscopy and abdominal computed tomography, did not show signs of occult tumours. The patient was diagnosed with idiopathic dermatomyositis and treated with systemic corticosteroids (methylprednisolone, 62.5 mg/day), azathioprine and methotrexate. Following 3 months of treatment, the cutaneous and muscular symptoms resolved and the patient is currently receiving maintenance therapy with azathioprine and methotrexate.

Export to PPT

Export to PPT

Export to PPT

Export to PPT
Export to PPT
Dermatomyositis is an uncommon autoimmune inflammatory myopathy of unknown aetiology. Patients may present with heterogeneous symptoms that can make diagnosis challenging. Pathognomonic rashes of dermatomyositis include Gottron’s papules and heliotrope rash. Symmetrical proximal muscle weakness or elevated muscle enzyme levels may help with the diagnosis.
Flagellate erythema is rare in patients with dermatomyositis, affecting <5% of cases.3 This skin condition is characterised by violaceous parallel streaks, also known as ‘zebra stripes’, often observed along with erythematous plaques. A pronounced erythematous hue indicates intense inflammation and an active disease state, distinguishing it from a bleomycin-induced condition that typically manifests as brownish and hyperpigmented lesions.1 Histopathological findings are non-specific; epidermal atrophy, vacuolar interface dermatitis, dermal oedema, mucin deposition and perivascular lymphocytic infiltration have been described.4 The evidence from direct immunofluorescence is inconclusive and the findings are controversial. Though the exact aetiology remains unknown, it is presumed to be associated with physical injury, such as minor trauma or sun exposure. Mechanical stimuli from recurrent scratching may also be a significant factor since pruritus is a common symptom.1 There are reports of an association with pulmonary complications or a paraneoplastic aetiology, especially in men.5 Therefore, these patients should be closely monitored for occult malignancies.
The gold standard therapy is systemic corticosteroids (prednisolone 0.5–2 mg/kg/day) in combination with topical corticosteroids or calcineurin inhibitors.6,7 Symptom relief is generally expected within 4 weeks, followed by gradual dose tapering.7 The use of antimalarial drugs like hydroxychloroquine is not recommended since it has recently been suggested to cause flare-ups of cutaneous disease.6 Disease-modifying antirheumatic drugs such as methotrexate, azathioprine, or mycophenolate mofetil can be administered as second-line or steroid-sparing agents. Other treatment options include rituximab, intravenous immunoglobulins and calcineurin inhibitors.
We present this case because of its distinctive morphology and unusual manifestations which contribute to the clinical heterogeneity of dermatomyositis.
Comments (0)