
Remember me
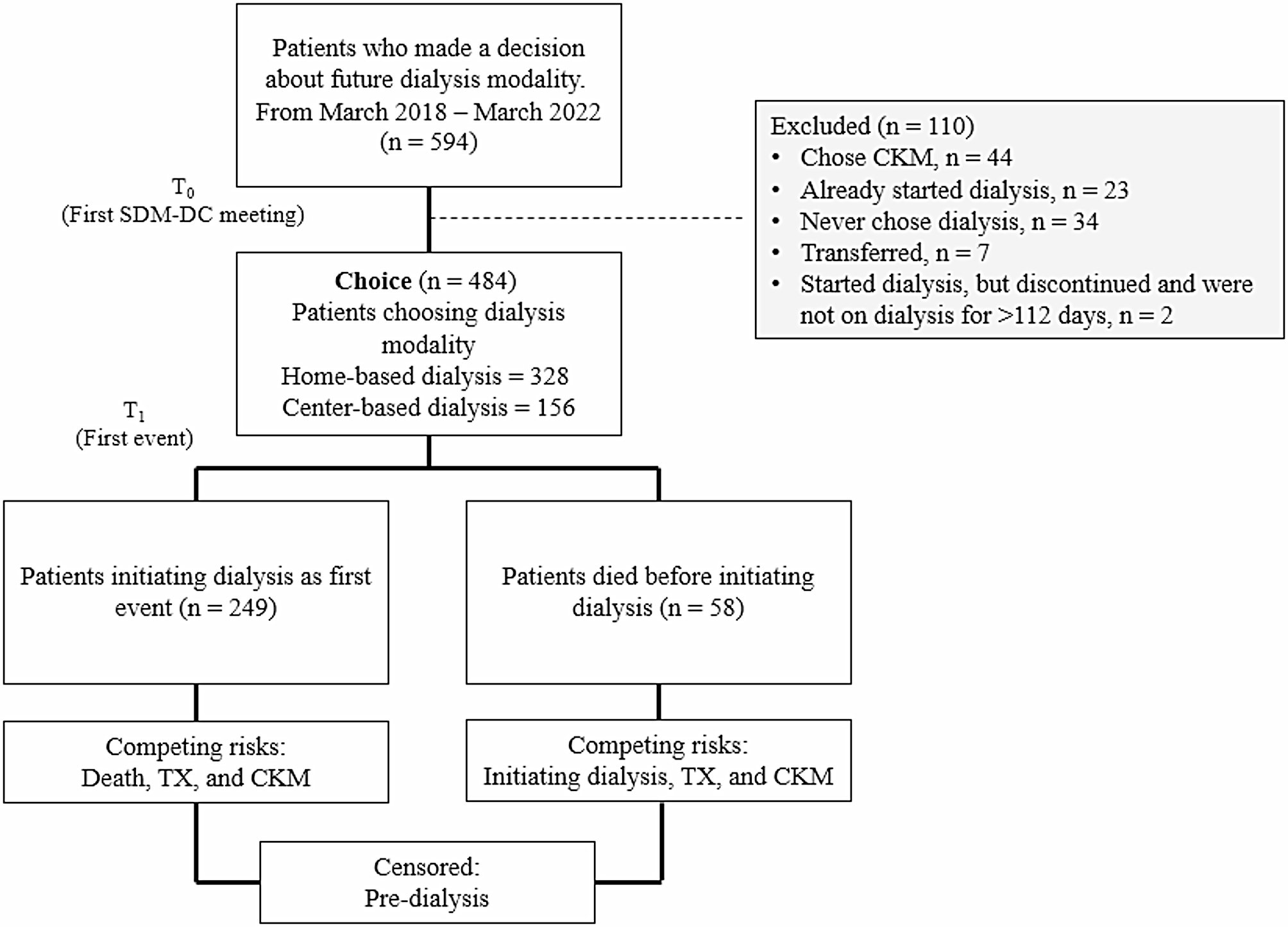






We identified all patients aged 18–80 years initiating dialysis from the United States Renal Data System (USRDS) [6], a national registry of all adults receiving kidney replacement therapy (KRT; either in the form of dialysis or transplant) for chronic kidney failure. We restricted our study sample to adults initiating dialysis Network 6 (Georgia (GA), North Carolina (NC), and South Carolina (SC)) between January 1, 2012 and March 13, 2017, and followed until December 2020. We restricted our cohort to 2012–2017 to ensure all patients had a minimum of 3-years of follow-up. We included patients who were pre-emptively referred or waitlisted (i.e., prior to dialysis initiation), and excluded patients from transplant facilities with missing referral dates. As the goal of this research is around setting reasonable goals of referral for dialysis facilities, we excluded all patients who received a transplant as their first KRT modality (i.e. pre-emptively transplanted patients). Our final study sample included 43,952 adults (Fig. 1). This study adheres to the STROBE guidelines for observational studies (Table S1).
Fig. 1
Flowchart of study population, incident dialysis patients from GA, SC, NC, 2012–2017. Abbreviations: CKD chronic kidney disease, E-STAR Early Steps to Transplant Access Registry, GA Georgia, NC North Carolina, SC South Carolina, USRDS United States Renal Data System
Study outcomes – referral and waitlistingOutcome data were obtained by linking individuals in the USRDS cohort to patient-level referral data obtained from the Early Steps to Transplant Access Registry (E-STAR), [1, 7] a voluntary registry of transplant referral and evaluation data collected from all (i.e., 100% capture) nine adult transplant centers in end-stage renal disease (ESRD) Network 6. Waitlisting data was obtained from USRDS. All individuals were followed from dialysis start date and followed through March 13, 2020 to allow for at least one year of follow-up to referral and at least two years of follow-up to waitlisting thereafter for all individuals. Two years was chosen as the time cut-off for waitlisting based on examination of the cumulative incidence of waitlisting that demonstrated that for the majority of patients who were waitlisted, they were waitlisted within 2-years of referral (see Figure S1). Specifically, approximately 29% of patients were waitlisted within 24 months, as compared with 36% (cumulatively) at 60 months (from time of referral). This was balanced with a smaller proportion of deaths occurring in this window (i.e., ~ 12% at 24 months vs. 29% at 60 months). For individuals who were pre-emptively referred or waitlisted (i.e., prior to dialysis initiation), follow-up time was calculated as 1-day. Referral was defined as date of first referral within 1-year of dialysis initiation. Waitlisting was defined as date of waitlisting within 2-years of referral date.
Patient-level covariatesPatient-level characteristics, as recorded in USRDS at time of dialysis start, were ascertained from the Centers for Medicare and Medicaid (CMS) form 2728. Key variables of interest included attributed cause of ESKD (diabetes, hypertension, glomerulonephritis, other), age (categorized as 18–29, 30–39, 40–49, 50–59, 60–69, 70 + years in models)), sex (men or women), race and ethnicity (non-Hispanic White, non-Hispanic Black, Hispanic, and ‘other,’ where other is made up of Middle Eastern, American Indian or Alaskan Native, Asian, Indian, Pacific Islander, and multi-racial), and dialysis type (hemodialysis, continuous ambulatory peritoneal dialysis (CAPD), continuous cycling peritoneal dialysis (CCPD) or other). Other variables of interest collected on the CMS2728 form included access to pre-kidney failure nephrology care (yes, no), comorbidities (tobacco use, congestive heart failure, diabetes, hypertension, atherosclerotic heart disease, other cardiac disease, cerebrovascular disease, peripheral vascular disease, cancer, chronic obstructive pulmonary disease (COPD), and obesity defined as body mass index (BMI) ≥ 35 kg/m2). Insurance status was defined as no insurance, Medicaid, Medicare, employer, or other. For health insurance status, where patients indicated they had > 1 insurance provider, we categorized them using a hierarchy of employer, Medicaid, Medicare, and other. In the US, Medicare is provided to all adults ≥ 65 years, individuals with disability, or individuals receiving treatment for kidney failure. Medicaid is provided to all individuals defined as low-income based on state-specific thresholds. For all non-primary variables, excluding pre-kidney failure nephrology care, < 5% of data were missing. For pre-kidney failure nephrology care, 13.1% of data were missing.
Statistical analysisDefining a ‘good’ transplant candidateTo estimate the proportion of patients with kidney failure not referred within one year who may have been good transplant candidates, we first defined ‘good transplant candidates’ as patients waitlisted within two years of referral date among those referred within 1-year from dialysis initiation.
Propensity Score (PS) developmentTo estimate the proportion of non-referred patients potentially eligible for referral the following stepwise process was used:
First, in order to identify ‘good’ transplant candidates, we performed a multivariate logistic regression in our cohort of patients referred within one year of dialysis initiation, using waitlisting within two years as the outcome of interest. We estimated the predicted probability (i.e., propensity score) of being waitlisted within two years of referral versus not being waitlisted within two years of referral by introducing explanatory clinical characteristics (age, attributed cause of kidney failure, and all patient-level comorbidities) based on a priori clinical knowledge. Type of insurance coverage, sex, and race/ethnicity were not included in the model since we only wanted to include factors that should be used to determine patient suitability for transplant in an ideal situation. A complete case approach was used as < 5% of data was missing across all variables included in models. The final model was used to estimate a PS for each patient.
Second, we evaluated the model's ability to distinguish between patients who were waitlisted within 2 years of referral and those who were not using the Area Under the Receiver Operating Characteristic curve (AUROC). To select the optimal PS cut-off for our model, we identified the threshold corresponding to the point closest to the top-left corner of the AUROC curve. This point balances sensitivity and specificity, providing an effective threshold for the model to accurately differentiate between waitlisted and non-waitlisted patients [8].
Third, we applied this PS logistic regression model to our non-referred cohort and selected the patients with a waitlisting probability within the above-mentioned PS cut-off (i.e., patients with a high predicted probability of waitlisting). We compared the clinical and demographic characteristics of these non-referred patients with those of referred patients to assess non-medical factors that might explain the remaining observed differences.
Sensitivity analysesGiven known disparities in who is and is not referred [1, 7], we also estimated PS for good transplant candidates among the entire dialysis cohort (vs. only among those referred in primary analysis). The same approach was taken as described above with some exceptions. Given all dialysis patients include those who were not referred, we no longer had a requirement of referral within 1-year plus waitlisted within 2 years of referral to define a good transplant candidate. Instead, for the total population we defined a good transplant candidate as someone who was waitlisted within 3 years of dialysis initiation. Three years was chosen to match primary analyses which included 1-year of referral plus 2-years of waitlisting. Furthermore, because referral was no longer a requirement to be a ‘good transplant candidate’, we did not define our referred and non-referred cohorts as referred (or not) within 1-year of dialysis initiation, thus sample populations are slightly different to those in primary analysis. The PS cut-off chosen to define a good transplant candidate in sensitivity analysis was similarly defined as above using AUROC curves.
Comments (0)