Test yourself: chest wall asymmetry
Lipomatosis of nerve, also called fibrolipoma or fibrolipomatous hamartoma of nerve, is defined as infiltration of a peripheral nerve by adipose and fibrous tissue [1]. Macroscopically, there is fusiform enlargement of the nerve due to adipose tissue, which is confined within the epineurium. It usually presents by early adulthood but can be detected at birth. The majority (85%) of these lesions have been described in the median nerve and its distal branches [2]. Another relatively common site is the ulnar nerve [3]. It is associated with overgrowth of tissue in a nerve territory in up to 67%, ranging from abnormal enlargement of digits (macrodactyly) to hemihypertrophy, with overgrowth of all mesenchymal elements referred to as macrodystrophia lipomatosa [4]. Activating mutations of the catalytic subunit of phosphatidylinositol 3-kinase (PI3KCA) (p.H1047R, p.H1047L, p.E545K, p.E542K and p.C420R) are frequent in lipomatosis of nerve irrespective of the location or degree of overgrowth: the term ‘PIK3CA-related lipomatosis of nerve’ has been proposed [5].
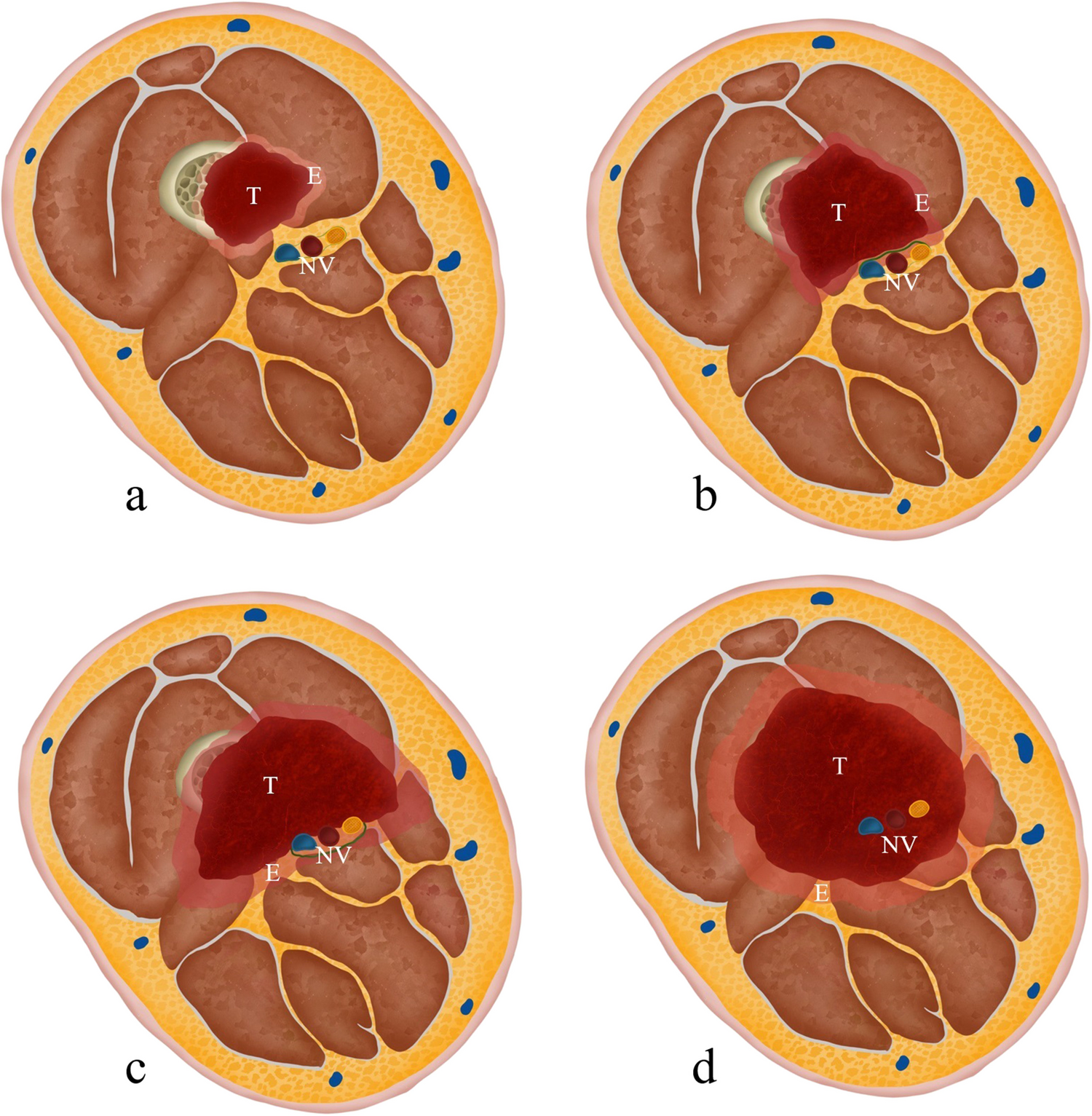
Classical imaging features of lipomatosis of nerve include hyperintense T1- and T2-weighted (adipose) signal evenly distributed between nerve bundles: the ‘co-axial cable’ appearance [6]. However, more recently, circumferential proliferation of fat around the epineurium of the nerve has been described [7]. The abnormally innervated bone can show osseous enlargement, ‘osteochondromatous proliferations’, hypertrophy and ankyloses of innervated joints [5] as demonstrated in our case.
Macrodystrophia lipomatosa has no gender predominance. Unilateral distribution is common, with distal extremity (hand or foot) involvement more common than the whole limb. A typical manifestation is unilateral foot involvement affecting the second and third toes [8]. The localised overgrowth may not be at the site of the mass but occurs in the distribution of the affected nerve. Cases outside the distal appendicular nerves are rare and include the tibial nerve [9], sciatic nerve [10] and abdominal wall [11]. In several of these cases, despite an unusual location of the nerve lipomatosis, typical limb deformity was still identified, for example such as digital enlargement due to mid-calf tibial nerve lipomatosis [9].
There is one previous report of axial nerve involvement, described as ‘segmental thoracic lipomatosis of nerve with nerve territory overgrowth’, with identical imaging features to the current case [12].
Differential diagnoses to consider include neurofibromatosis type 1 (NF1), parosteal lipoma/liposarcoma and Klippel-Trenaunay-Weber syndrome. The pathognomonic feature in lipomatosis of nerve is overgrowth of all the mesenchymal elements in the anatomical distribution of the affected nerve and histological confirmation is not necessary [12]. This lesion demonstrated stable clinical features and imaging appearances at 6 months. The patient was referred to a tertiary cardiothoracic centre for further management and was unfortunately lost to follow-up at our hospital.




Comments (0)