
Remember me



This retrospective, single-center study was approved by the Institutional Review Board (Ethics Committee number KCRC-21-0037). The requirement for informed consent was waived owing to the retrospective nature of the study.
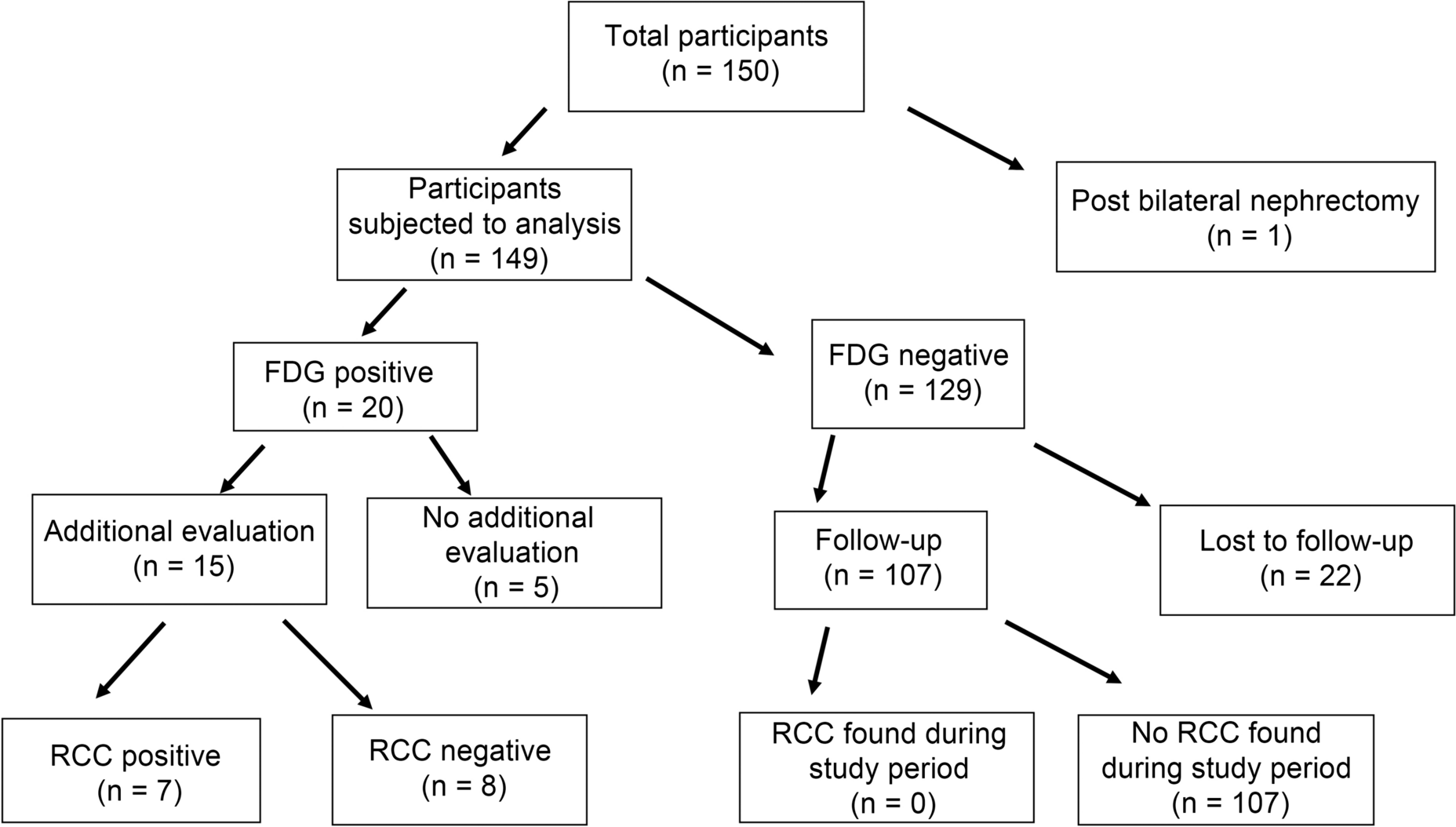
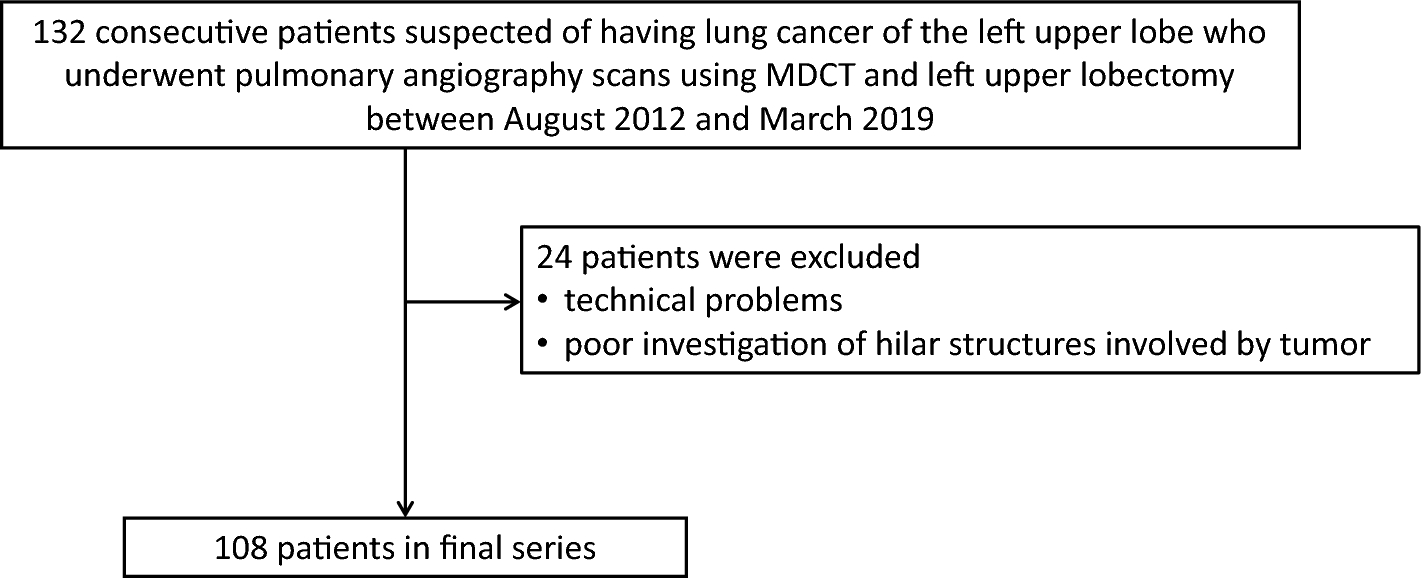
Patients with ILD who underwent thoracoscopic SLB between October 2018 and January 2022 were eligible (Fig. 1). We included 122 consecutive patients with fibrosing ILD who underwent CT examinations within 6 months before surgery. Patients with lung cancer (n = 12) and pulmonary infection (n = 3) were excluded, because these involve neoplastic cell proliferations. The patients who previously underwent thoracic surgery (n = 4), one with a foreign body in the lung (n = 1) and two with inadequate CT image quality (n = 2), were also excluded because of the potential undesirable artifacts. Baseline clinical measurements, including pulmonary function tests, were obtained within 3 months of the CT examinations. All baseline CT images were non-contrast, obtained using a thin-slice CT scanner (Aquilion Precision, Canon Medical Systems, Otawara, Japan) at full inspiration in the supine position with a tube voltage of 120 kVp and automatic tube current modulation. The median effective dose (interquartile range) of the CT scans was 8.23 (7.24–9.1) mSv. These data were calculated based on the dose–length products (mGy · cm) and a k-factor of 0.0140 (mSv · mGy−1 · cm−1). We used the CT images reconstructed using filtered-back projection and soft kernel, with 512 × 512 matrices and 0.5 mm slices. We automatically measured the total lung volume and the extent of each lesion using artificial intelligence-based software [Quantification by Ziosoft Informatics Platform for Interstitial Lung Disease (QZIP-ILD), Ziosoft, Tokyo, Japan] [17]. Two board-certified chest radiologists performed IPF and HP pattern classification according to the American Thoracic Society guidelines [1, 4] without clinical and pathological information. The findings were agreed upon in a consensus between the two radiologists.
Fig. 1
Study flowchart. SLB, video-assisted thoracic surgery; SLB, surgical lung biopsy
Biopsy and histopathological/morphometrical analysisOne pathologist with 20 years of experience in ILD selected a representative hematoxylin–eosin-stained slide for each SLB site. The slides were scanned using a virtual slide scanner (NanoZoomer, Hamamatsu Photonics, Hamamatsu, Japan). Then, we counted the number of nucleated cells and measured the tissue area using public morphometric software (QuPath v0.2.3) [18]. We calculated the number of nucleated cells per unit area (1000 μm2). Among specimens from the 99 patients with two SLB sites, those with the higher cell count were used for the analysis. We compared the cell counts between patients treated with and without anti-inflammatory therapy. A multidisciplinary discussion (MDD) that included specialists in respiratory medicine, diagnostic radiology, and pathology determined whether anti-inflammatory therapy was indicated. Based on a comprehensive review of the patient's clinical course, encompassing a detailed chronological medical history, thorough physical examination, and a series of laboratory and imaging tests subsequent to the initial diagnosis of MDD, the diagnosis of unclassifiable disease was revised during the departmental conference in respiratory medicine.
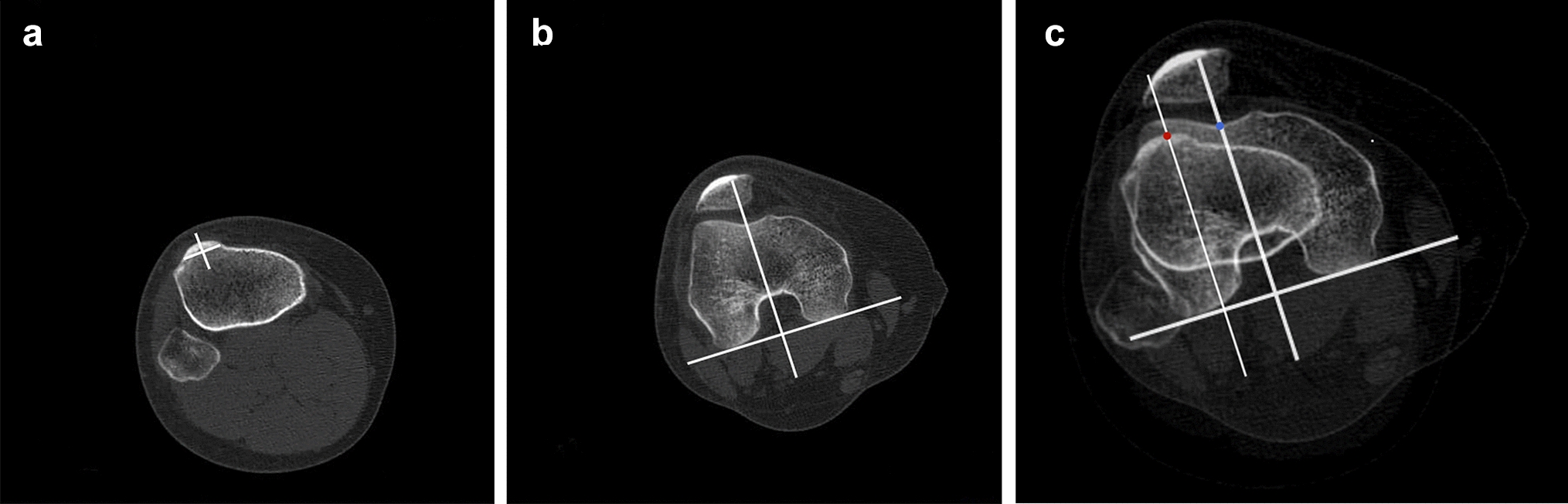
Radiomics analysis and radiomics-based modelsA schematic diagram of the region-of-interest (ROI) placement and construction of the specimen-based model and patient-based model is shown in Fig. 1. We positioned the ROI using surgical staples as a guide to indicate the biopsy site. The staple line measured 2–4 cm in length in the post-operative CT images. Therefore, we placed two volumes of interest (VOIs) to cover the staple line. Moreover, we measured the radiomics features. All VOIs were placed by an expert radiologist with 29 years of experience or a pneumologist with 18 years of experience. The center points of the two spherical VOIs with 2 cm diameter were manually placed to include a maximum volume of the interstitial lesion, as well as the portion removed by SLB in each patient. In usual interstitial pneumonia (UIP) pattern fibrosis, the lesion existed just below the pleura. Therefore, VOIs included some extrapulmonary regions. When the sphere contained extrapulmonary regions, these regions were automatically removed using QZIP-ILD [17]. All radiomics features were calculated using in-house software based on PyRadiomics (version 3.0.1; https://pyradiomics.readthedocs.io/en/latest/). In total, 107 radiomics features from the category of the histogram and gray-level co-occurrence matrix were extracted from each VOI and the whole lung.
The radiomics features obtained from the two VOIs placed for each SLB site were labeled as “SLB.a” and “SLB.b.” The order of labeling was arbitrary. Radiomics features extracted from regions obtained from whole lungs were labeled “_WL.” We built two radiomics-based models. One model predicts cell counts in the histological specimens (specimen-based model) with “SLB.a” and “SLB.b.”-labeled radiomics features, and another one predicts patients with abundant cellular infiltration in their histology specimens (patient-based model) with “SLB.a”, “SLB.b.” and “WL.”-labeled radiomics features.
Step-1: relationship of specimen-based model and histological cell countTo build the specimen-based model, 199 VOIs were divided into two datasets: training (140 specimens) and validation (59 specimens). A linear regression model with the least absolute shrinkage and selection operator (LASSO) [19] was applied to simultaneously construct a support vector machine (SVM) to predict the number of cells per unit area in surgical specimens and select significant radiomics features in the training dataset. A discordant pathological diagnosis between different biopsy sites is frequently observed in the same patient [20]. Therefore, we treated the specimens obtained from different biopsy sites in one patient as different samples.
Step-2: relationship of patient-based model and the dichotomized classification of cellularityIn clinical settings, the level of cellularity, whether high or low, is one of the crucial factors in justifying the indication for an anti-inflammatory therapy. Therefore, the patient-based model to classify the patient to high or low cellularity was developed. We divided patients into two groups, one with high cell counts and the other one with low cell counts. The median value of the histological cell counts across all patients was used to define the cut-off value to dichotomize the degree of cellularity: 50 high-cellularity cases and 50 low-cellularity cases. Seventy of these 100 cases were randomly selected and used as training datasets to build the model. Thirty separate cases were used as test data for external validation. We constructed this model using SVM with LASSO, the same as for the specimen-based model in Step 1.
Statistical analysisContinuous patient characteristics are summarized using descriptive statistics (n, mean, median, standard deviation, and interquartile range), while categorical patient characteristics are summarized using frequency (percentage). The histological cell counts were compared between the two groups, i.e., the anti-inflammatory therapy group and the non-anti-inflammatory therapy group, using Student’s t test.
In the specimen-based prediction model, for the evaluation of the relationship between the actual and predicted number of cells, the estimated model was evaluated using a root-mean-square error in the validation dataset, and the correlation coefficient (R) and p value of the linear fit were calculated. The R package ‘glmnet’ (https://cran.r-project.org/) was used for the model construction.
In the patient-based prediction model, the median cell count was used as a cut-off to classify patients into two groups, and the model was constructed using the R package ‘glmnet’. The model’s performance was evaluated by the F1 score and the accuracy of the result of validation.
To compare the radiomics features between the specimen-based and patient-based models, the top five features in regression coefficient value were selected for each of the specimen-based model and patient-based model in the order of absolute value, and a heat map was created to show the correlation between them.
Comments (0)