
Remember me
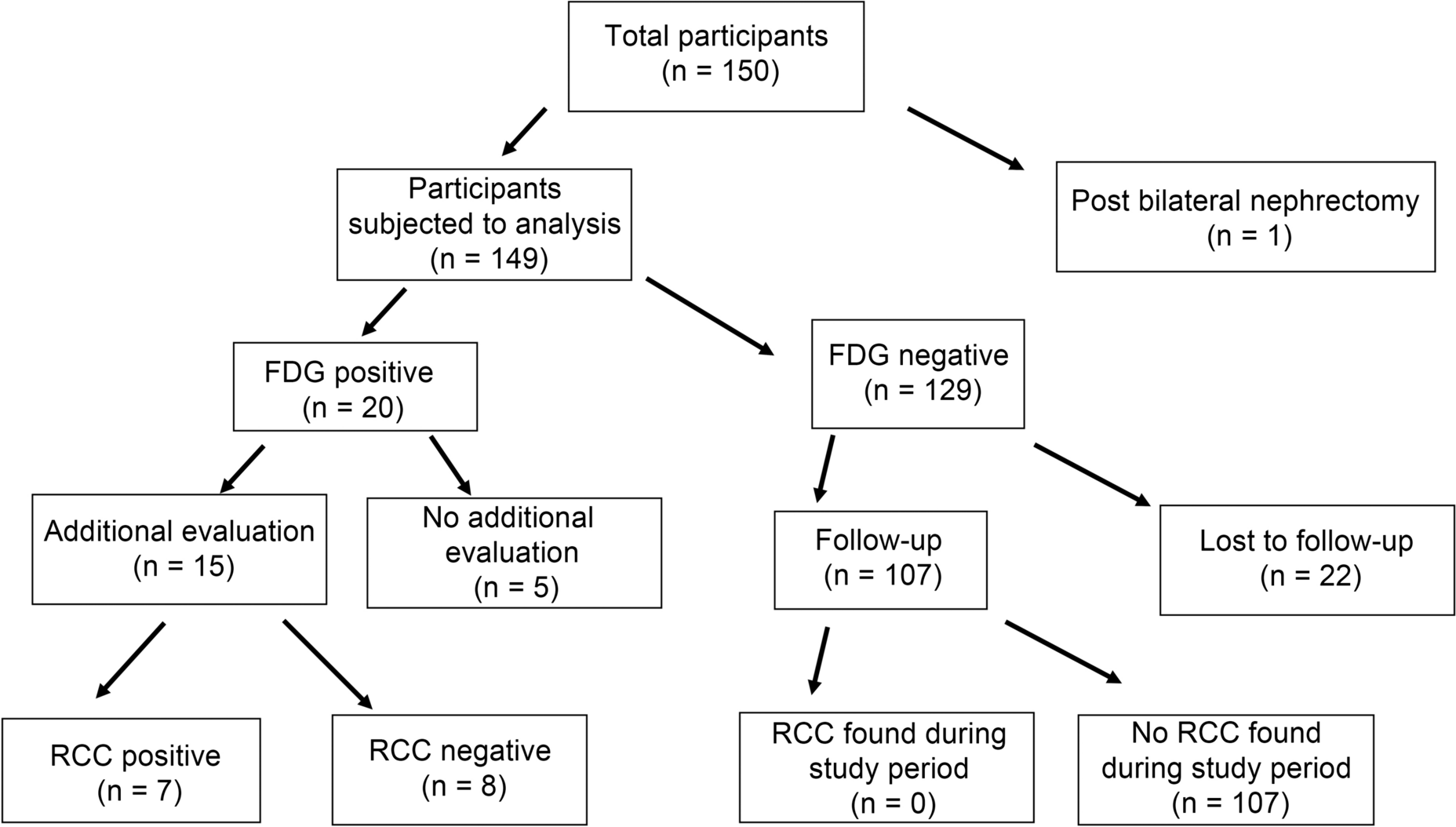


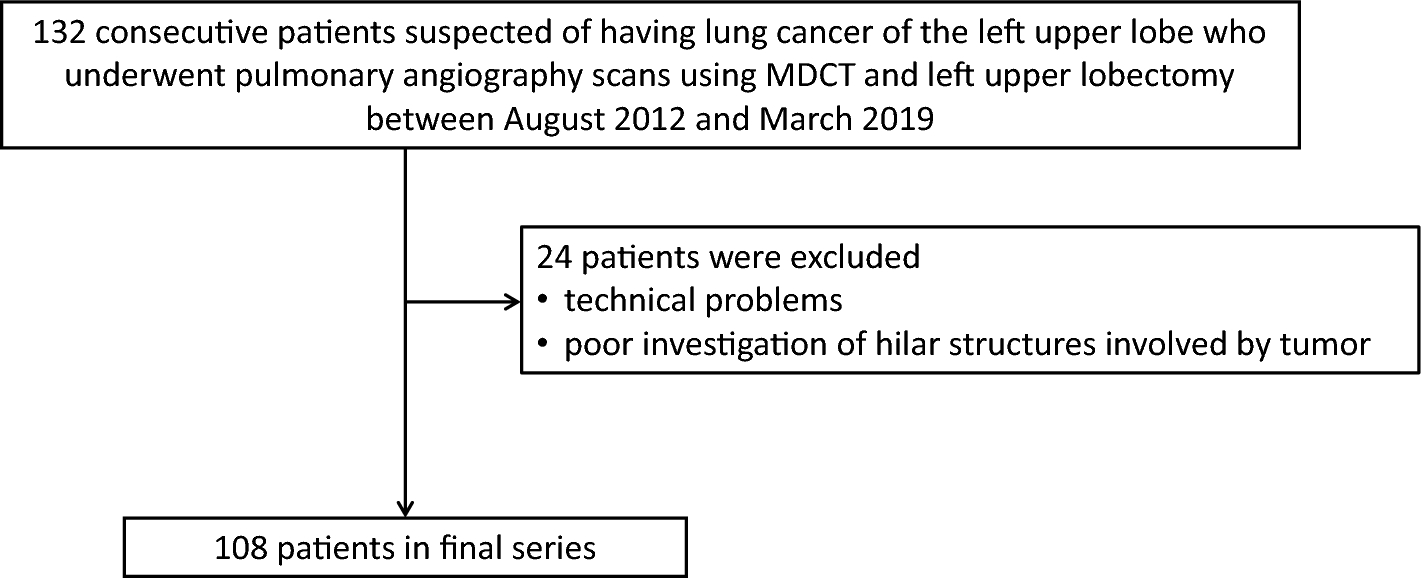

This prospective study was approved by the Institutional Review Board of our institution (No. 5215). Written informed consent was obtained from all participants. Between July 2021 and June 2023, 81 consecutive patients who underwent 99mTc-GSA scintigraphy as preoperative examination for hepatectomy were enrolled in this study. The initial inclusion criteria were as follows: (1) patients who underwent segmentectomy or more and (2) patients who underwent ICG clearance test as a preoperative examination and contrast-enhanced CT as pre-and postoperative examinations. From the initial population, patients who met the following criteria were excluded from the analysis: (1) patients who did not undergo hepatectomy after preoperative examination and (2) patients who had reasons that might affect the PHLF criteria, as described below (Fig. 1).
Fig. 1
Flowchart of the study. 99mTc-GSA Technetium-99m-galactosyl human serum albumin
Imaging protocols of 99mTc-GSA SPECT/CTSPECT/CT images were obtained using an SPECT/CT scanner (Symbia T6, Siemens Healthineers, Erlangen, Germany) with a dual-head gamma camera and low-energy, high-resolution collimators. After an overnight fast, 99mTc-GSA (Nihon Medi-Physics Co., Ltd., Tokyo, Japan) at a mean dose of 266.1 MBq (range 123.4–304.9 MBq) was injected intravenously. SPECT images (step-and-shoot, 90 steps of 25 s/step, 360°, and 128 × 128 matrix) were obtained 20 min after 99mTc-GSA injection. A low-dose CT scan (helical, 130 keV, 70 mAs, and 2.5 mm slice thickness) was performed for attenuation correction. SPECT and CT images of the entire liver were obtained. The SPECT images were reconstructed using an ordered subset expectation maximization algorithm (five subsets, nine iterations) and a Gaussian filter (FWHM = 8.0 mm).
Image analysis of 99mTc-GSA SPECT/CTThe SPECT/CT images were analyzed using the free software RAVAT version 1.00 (Nihon Medi-Physics Co., Ltd., Tokyo, Japan). First, a cubic volume of interest (VOI) containing the entire liver was created. Then, the software automatically detected the region of voxel with SUV ≥ 20. The threshold was determined to match liver contours. SUV was calculated using the following formula: SUV = total radioactivity of the VOI (Bq/mL)/[injected dose (Bq)/body weight (g)]. The software automatically measured liver volume segmented above threshold (SUV ≥ 20) (Fig. 2). Liver volume was defined as the functional liver volume of total liver (t-FLV).
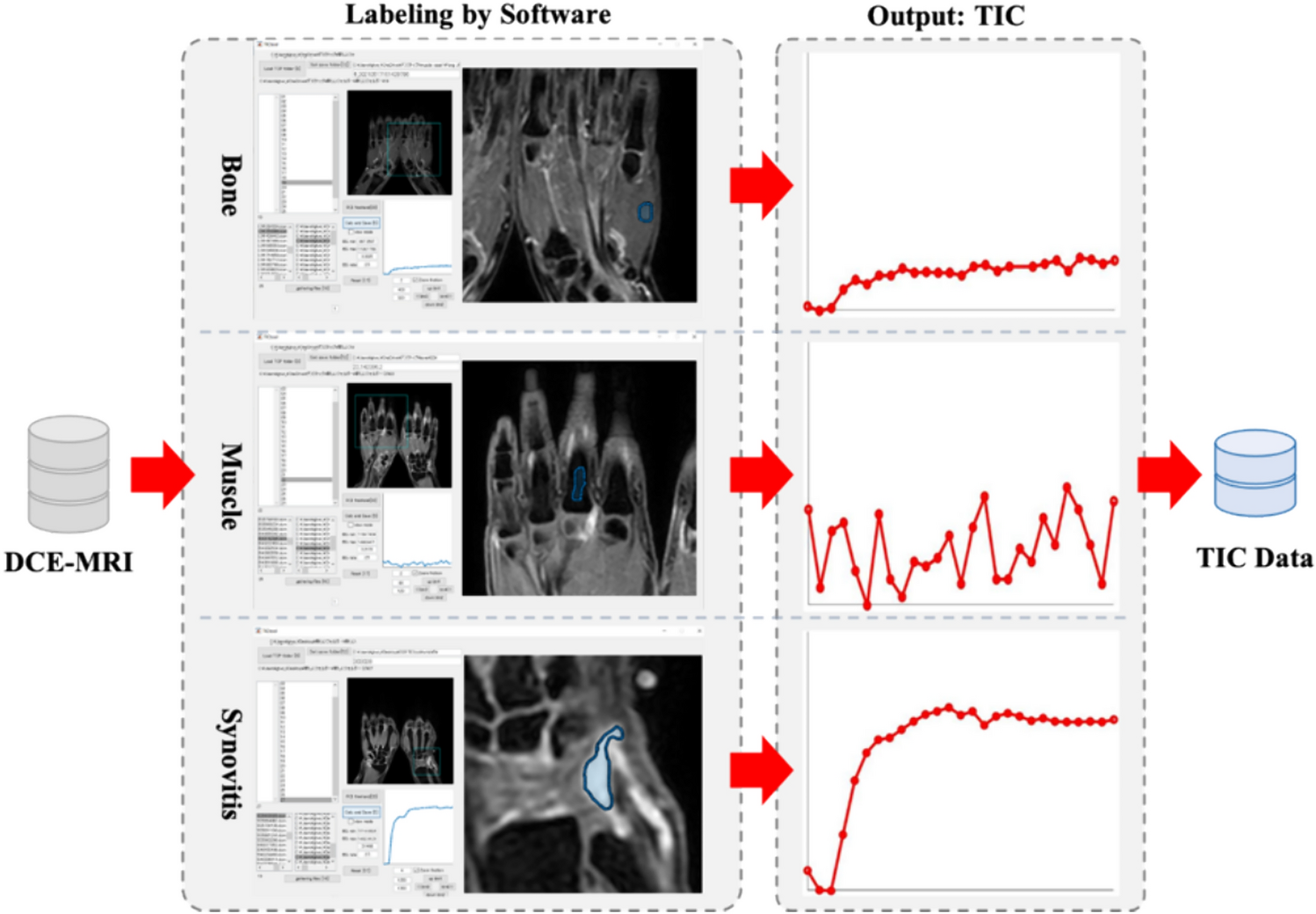
Fig. 2
Calculation of functional liver volume of total liver (t-FLV) and functional liver volume of remnant liver (r-FLV) for left lateral sectionectomy. a (Transaxial image), b (coronal image), and c (sagittal image) show calculation of t-FLV (yellow line). The software (RAVAT) automatically contoured whole liver above standardized uptake value (SUV) ≥ 20. d (Transaxial image), e (coronal image), and f (sagittal image) show calculation of r-FLV (orange line). The resection line was drawn manually
The resection line was determined with reference to the hepatic portal and hepatic veins on SPECT/CT images and pre-and postoperative contrast-enhanced CT images. The resection line was determined by consensus of two board-certified radiologists included in the study (Y.O., 11 years of radiology experience; S.Y., 22 years of radiology experience). Based on the resection line, the FLV of the remnant liver (r-FLV) was measured using RAVAT (Figs. 2 and 3).
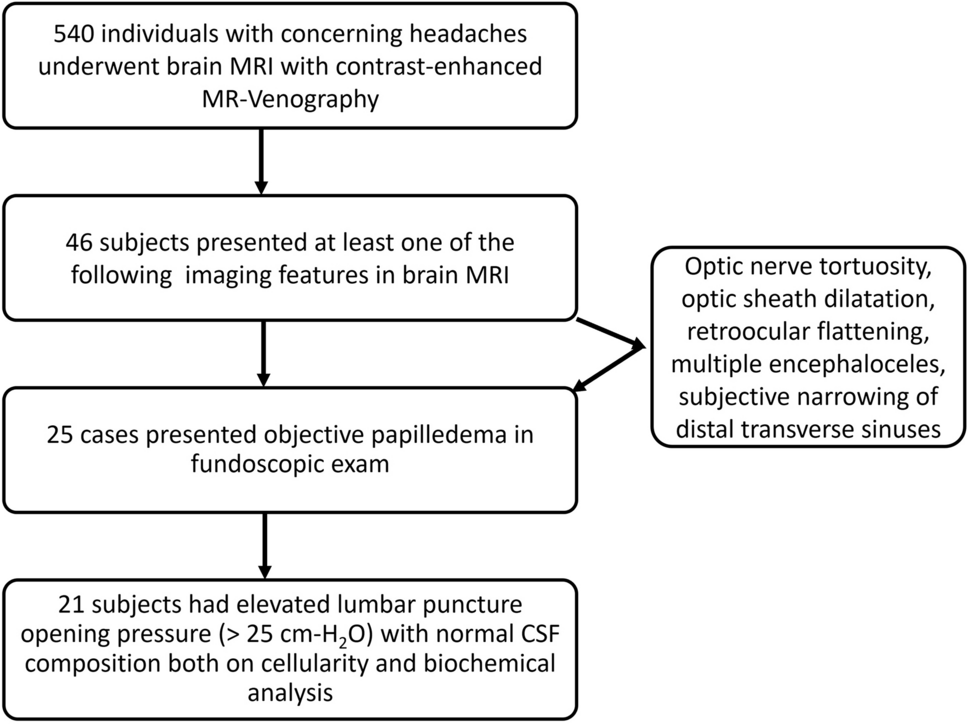
Fig. 3
Difference between single-photon emission computed tomography (SPECT) and CT contours in case of right hemihepatectomy after portal vein embolization for right branch of portal vein. In this case, liver accumulation was low, and SPECT contour of remnant liver (yellow line) was located inside CT contour (orange line)
Radioactivity in the syringe before and after injection, the time before and after injection, and body weight were recorded to calculate the SUV. A cross-calibration factor was calculated using a phantom to convert the SPECT count into a radioactivity value.
Imaging protocols and analysis of CTDynamic contrast-enhanced CT was performed using a 256-row CT scanner (Revolution CT, GE Healthcare, Chicago, IL, USA). The tube voltage was 120 kVp and the reconstruction thickness was 1.25 mm. A nonionic iodinated contrast agent (Iopamiron 370, Bayer Healthcare, Berlin, Germany) was administered intravenously. The total dose of the contrast agent was 100 ml and the injection rate was 3 ml/s. Images were obtained before injection and 34, 40, 46, 67, and 135 s after injection initiation. One patient received pre-injection and 40 and 135 s after injection initiation. Images at 67 s or 135 s after injection were used to determine resection line, because portal vein and hepatic vein were clearly enhanced. Total liver volume (t-LV) and remnant liver volume (r-LV) were measured using the AW Server software, version 3.2 (GE Healthcare, Chicago, IL, USA).
ICG clearance testThe ICG clearance test was performed as follows. A dose of 0.5 mg/kg ICG was administered intravenously, and blood was sampled before and at 5, 10, and 15 min after ICG administration. ICGK was determined using regression analysis.
ICGK-F was calculated using the following formula: ICGK × r-LV/t-LV. In addition, the ICGK × r-FLV and ICGK × r-FLV/t-FLV ratios were calculated.
Preoperative and postoperative dataEtiology of liver disease was obtained from electronic medical record. Preoperative serum levels of total bilirubin, albumin, aspartate aminotransferase, alanine aminotransferase, international normalized ratio of prothrombin time (PT-INR), and platelet counts were recorded. Postoperative serum total bilirubin and PT-INR levels were recorded daily after hepatectomy. The type of hepatectomy, the results of the pathological diagnosis, and presence or absence of cirrhosis in the background liver were recorded.
Preoperative managementIf the future remnant liver volume was insufficient, portal vein embolization (PVE) or associated liver partition and portal vein ligation for staged hepatectomy (ALPPS) was performed. PVE was performed when future remnant liver volume was less than 40% of the total liver volume on CT. ALPPS was performed when the future remnant liver volume was less than 30% of the total liver volume on CT volumetry, and the interval to hepatectomy was shortened. 99mTc-GSA scintigraphy, ICG clearance test, and contrast-enhanced CT were repeated within 1 month after PVE or ALPPS. Hepatectomy was planned again if the future remnant liver volume was > 40% of the total liver volume on the CT. Contrast-enhanced CT and SPECT/CT of post-PVE or ALPPS were used to calculate t-LV, r-LV, t-FLV, and r-FLV.
Definition of PHLFPHLF was defined according to the criteria of the International Study Group of Liver Surgery (ISGLS) as increased PT-INR and hyperbilirubinemia on or after postoperative day 5 [20]. The cut-off values of PT-INR and serum total bilirubin level at our institute were 1.15 and 1.50 mg/dl, respectively. If the PT-INR or serum total bilirubin level increased preoperatively, PHLF was defined as increased PT-INR and hyperbilirubinemia on or after postoperative day 5 (compared with the values on the previous day). The severity of PHLF was graded based on its impact on clinical management. Grade A was defined as PHLF that did not require any changes in the clinical management of the patient. Grade B was defined as PHLF requiring noninvasive treatment. Grade C was defined as PHLF requiring an invasive treatment.
Statistical analysisContinuous variables were expressed as medians (interquartile ranges). Continuous variables were compared between the PHLF and non-PHLF groups using the Mann–Whitney U test, and categorical variables were compared using Fisher’s exact and Chi-squared tests. Receiver-operating characteristic (ROC) curves were derived, and the area under the curve (AUC) was calculated to examine the diagnostic performance for predicting PHLF in ICGK-F, r-FLV, r-FLV/t-FLV, ICGK × r-FLV, and ICGK × r-FLV/t-FLV, respectively. The cut-off value was determined as the point closest to the upper-left corner of the ROC curve. The sensitivity and specificity of the PHLF were calculated using this cut-off value. Sensitivity and specificity for increased PT-INR or hyperbilirubinemia after hepatectomy in ICGK-F, r-FLV, and ICGK × r-FLV were calculated using the cut-off value for PHLF to examine whether synthetic reserve or excretory reserve was more influential in each index predicting PHLF. The bootstrap method with 2000 bootstrap samples was used to compare the area under the curve (AUC) values and to calculate the 95% confidence interval (CI) for sensitivity and specificity.
Statistical significance was considered when p value was less than 0.05 or 95%CI did not overlap. Statistical analysis was performed using the Bell Curve for Excel (Social Survey Research Information Co., Ltd., Tokyo, Japan) and R version 4.2.2.
Comments (0)