
Remember me
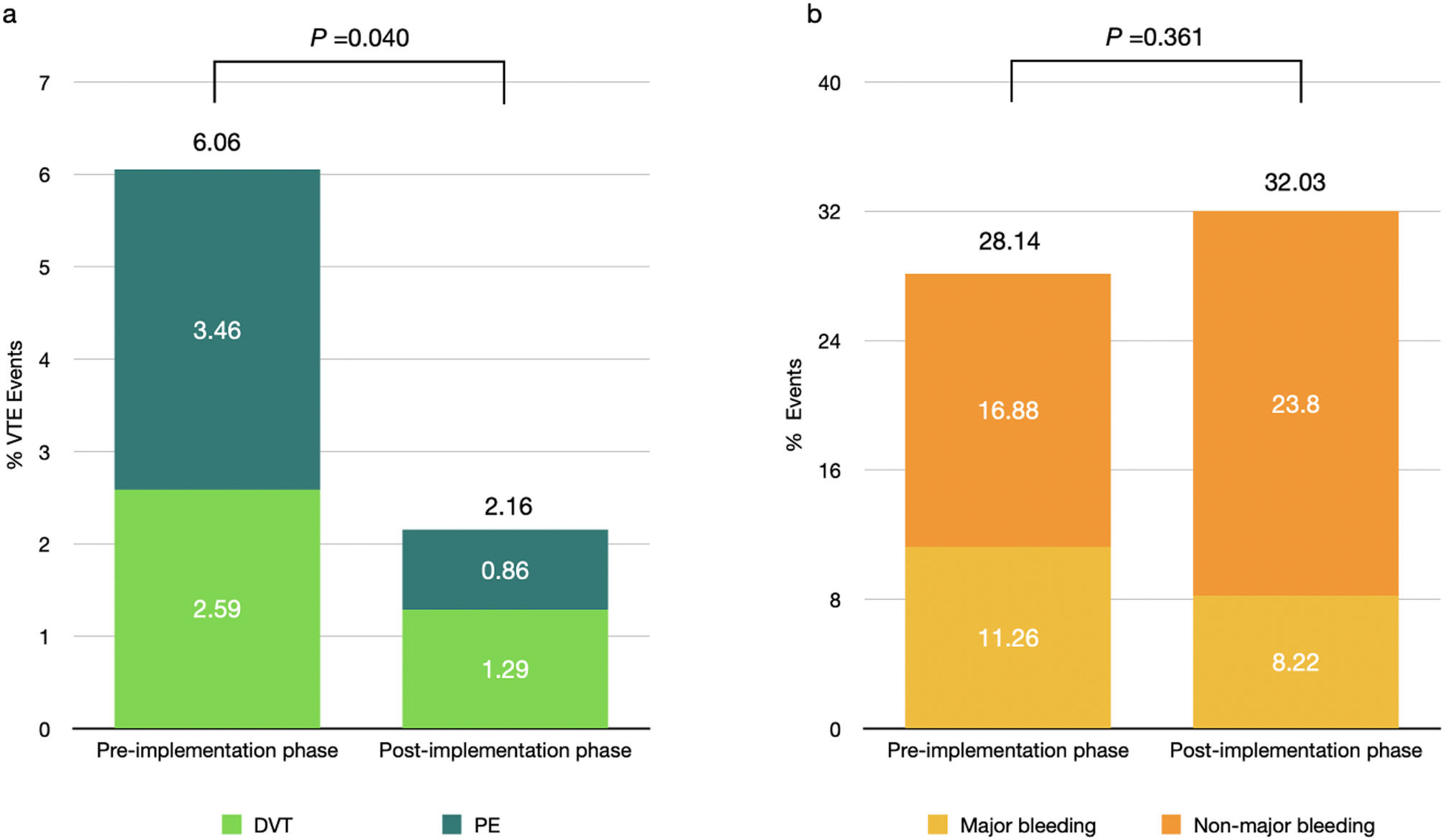

We obtained 8991 articles through preliminary screening. Duplicate and irrelevant articles were deleted. Six hundred and three articles were evaluated in full text, with 8 articles assessed as eligible but not used in data extraction (n = 8). Five hundred and eighty articles were excluded, including inappropriate population (n = 445); no drugs of interest (n = 44); no relevant outcomes (n = 23); subgroup analysis not of interest (n = 58); not a randomized controlled trial (n = 10). Finally, 23 articles were included for meta-analysis, including data from 25 trials (Fig. 1, Table 1).
Fig. 1
Study flow chart
Abbreviations: VTE, venous thromboembolism; RI, renal insufficiency
Table 1 Summary of studies included in meta-analysisIn the treatment of the acute phase, five trials involving 1759 patients compared the efficacy and safety between NOACs and VKA [18,19,20,21,22]. Two trials compared the efficacy and safety between LMWH and VKA [23, 24]. The Innohep® in Renal Insufficiency Study (IRIS) compared the efficacy and safety between LMWH and UFH [25]. Three trials compared the efficacy and safety between NOACs and LMWH [26,27,28].
In the treatment of the extension phase, EINSTEIN-CHOICE compared the efficacy and safety of two dosages of NOACs with those of aspirin for up to 1 year after the initial 6 to 12 months of therapy [29]. RE-MEDY and RE-SONATE compared the effectiveness of NOACs vs VKA and NOACs vs placebo [20]. Two trials investigated the efficacy and safety of NOACs vs placebo [30, 31]. Moreover, AMPLIFY-EXT also compared the efficacy and safety of low-dose NOACs vs placebo [30].
For VTE prophylaxis, four trials were included to analyze the safety and efficacy of NOAC and LMWH [32,33,34,35]. One trial compared the safety and efficacy between desirudin and LMWH [36]. Three trials investigated the effectiveness of NOACs versus placebo [37,38,39]. One trial compared the efficacy and safety of LMWH vs UFH [40].
Comparisons of different anticoagulants among patients with RIVTE treatment in the acute phaseIn the acute phase, a total of 3,475 VTE patients with RI were involved from eleven studies. Four pairs of comparisons were analyzed: NOACs vs VKA, LMWH vs VKA, LMWH vs UFH and NOACs vs LMWH. Among all the pairs, efficacy endpoints were not significantly different. For safety outcomes, NOACs were associated with an increased risk of bleeding compared to LMWH (RR 1.29, 95%CI 1.04–1.60). No significant difference was observed in the other pairs of comparisons (Fig. 2).
Fig. 2
Comparisons of Different Anticoagulants among Patients with RI in Forest Plot
Abbreviations: NOAC, novel oral anticoagulants; VKA, vitamin K antagonist; LMWH, low molecular heparin; UFH, unfractionated heparin
VTE treatment in the extension phaseA total of seven studies with 668 VTE patients with RI were enrolled in the extension phase. Five pairs of comparisons were analyzed: NOACs vs aspirin, low-dose NOACs vs aspirin, NOACs vs VKA, NOACs vs placebo, and low-dose NOACs vs placebo. However, no statistically significant difference of efficacy was detected.
For safety outcomes, the placebo was at a lower risk of bleeding than low-dose NOACs (RR 1.64, 95%CI 1.03–2.62), while no significant difference was shown in other comparison pairs (Fig. 2).
VTE prophylaxisThe analysis of VTE prophylactic phases contained nine studies involving 5,537 VTE patients with RI. Four pairs of comparisons were analyzed: NOACs vs aspirin, low-dose NOACs vs aspirin, NOACs vs VKA, NOACs vs placebo and low-dose NOACs vs placebo. Compared with LMWH, desirudin was associated with a lower risk of VTE occurrence (RR 0.71, 95%CI 0.51–0.98) but a higher risk of bleeding (RR 1.49, 95%CI 1.00–2.24) Meanwhile, NOACs significantly increased the risk of bleeding compared with placebo (RR 1.31, 95%CI 1.02–1.68) (Fig. 2).
Efficacy and safety of different anticoagulants among patients with and without RIWe also conducted meta-analyses on participants with and without RI who had been prescribed each anticoagulant, to investigate the efficacy and safety of one particular anticoagulant in both populations.
VTE treatment in the acute phaseIn the acute phase of the treatment studies, a total of 2,938 VTE patients with RI and 28,161 VTE patients without RI were included. Three anticoagulants were analyzed: NOACs, VKA, and LMWH. Among the seven studies using VKA, the risk of death or recurrent VTE was significantly higher in the RI patients (RR 1.43, 95%CI 1.13–1.82). For safety outcomes, NOACs and VKA might lead to a higher risk of bleeding among the RI patients compared with those without RI (RR 1.45, 95%CI 1.14–1.84 and RR 1.53, 95%CI 1.25–1.88, respectively) (Fig. 3).
Fig. 3
Effects of Different Anticoagulants among Patients with and without RI in Forest Plot
Abbreviations: NOAC, novel oral anticoagulants; VKA, vitamin K antagonist; LMWH, low molecular heparin.
VTE treatment in the extension phaseIn the extention phase of the treatment studies, a total of 559 VTE patients with RI and 10,474 VTE patients without RI were included. Five anticoagulants were analyzed: NOACs, aspirin, low-dose NOACs, VKA and placebo. The efficacy of these drugs between RI and non-RI patients was found to be similar. Aspirin may increase the risk of bleeding in RI patients (RR 3.21, 95%CI 1.28–8.09) (Fig. 3).
VTE prophylaxisIn the VTE prophylaxis studies, a total of 4,933 VTE patients with RI and 22,910 VTE patients without RI were included. Four anticoagulants were analyzed: NOACs, LMWH, desirudin and placebo. Compared with the non-RI population, NOACs may increase the occurrence of VTE in RI population (RR 1.74, 95%CI 1.29–2.34). There was no difference among groups treated with NOACs, placebo and desirudin, but LMWH could increase the risk of bleeding in the RI population (RR 1.33, 95%CI 1.01–1.75) (Fig. 3).
Comments (0)