This report has two important clinical teaching points: (1) ACS can occur as a complication of endoscopic carbon dioxide insufflation and (2) ACS should be suspected if a sudden change in level of consciousness or respiratory disturbance occurs during endoscopic procedure in a patient with malignant bowel obstruction.
Colonic stenting as a bridge to surgery is recommended as one of the treatment options for malignant colonic obstruction in the European guidelines [3]. However, while colonic stenting is considered a relatively safe procedure, the stent-related mortality rate is approximately 1% [9], and complications that require emergency surgery, such as colonic perforation, occur in 3.7% to 4.8% of cases [6, 9,10,11]. Therefore, candidates for colonic stenting should be selected carefully, given that they are often already in poor condition.
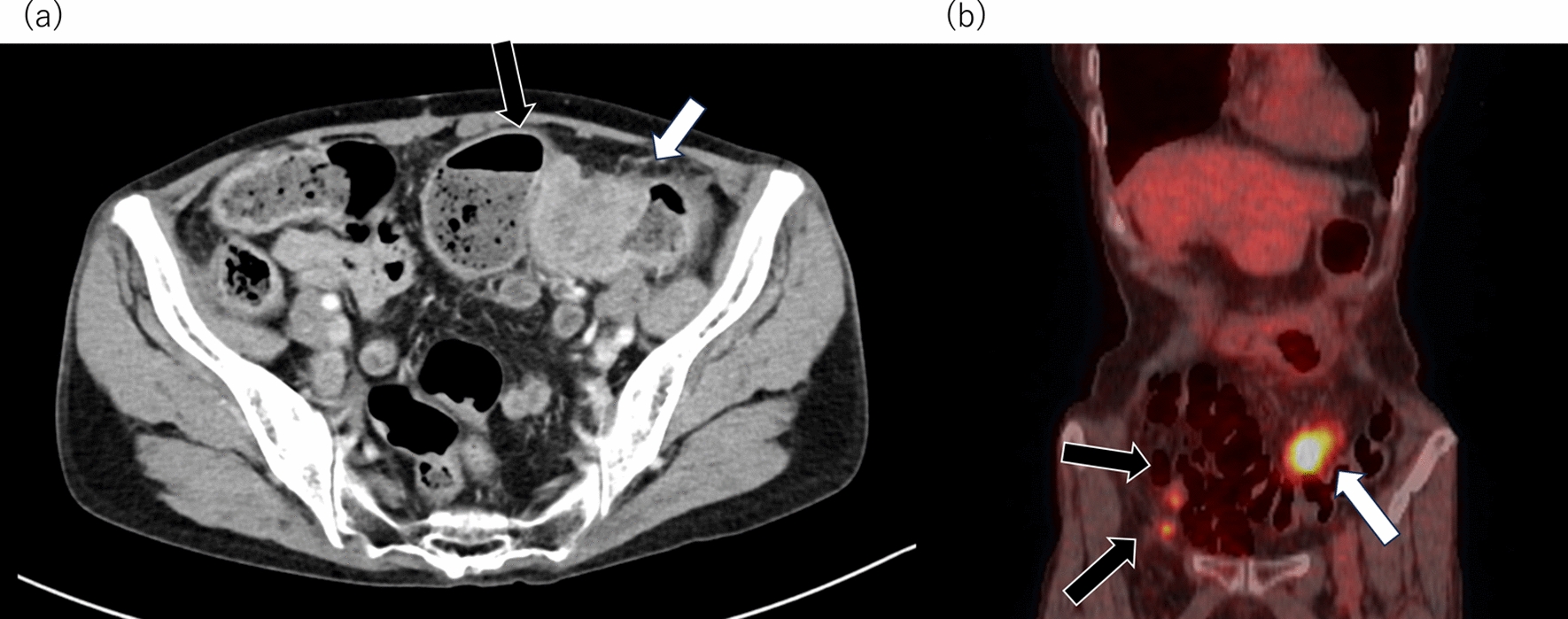
This is the first report of ACS as a complication of endoscopic insufflation during colonic stenting. In this case, the sigmoid colon cancer acted as a one-way valve, trapping the air delivered by the colonoscope and causing remarkable intestinal dilation and pneumoperitoneum without perforation, resulting in ACS. Pneumoperitoneum has been reported to occur at rates of 0.3%–1% in diagnostic colonoscopy and 3% in therapeutic colonoscopy [12]. Most cases of pneumoperitoneum without perforation do not require surgical intervention; however, there has been a report of a case of ACS caused by pneumoperitoneum without perforation [13]. In patients with malignant colonic obstruction, intra-abdominal pressure can be high even before colonoscopy is started; therefore, careful attention to air delivery is needed during colonic stenting.
Perforation at the time of stent insertion is a major complication requiring surgery and often manifests as abdominal pain or subcutaneous emphysema one hour to one day later [6, 14]. However, in a case of ACS, acute respiratory failure and a change in consciousness occurs during the procedure. Therefore, ACS should be suspected when these changes occur during stent insertion. Marked abdominal dilatation on physical examination is important for diagnosis, and pneumoperitoneum without contrast leak on CT may be a useful finding.
ACS is usually caused by rapid addition of volume [15], in which case primary abdominal closure after decompressive laparotomy is often difficult [7, 16, 17]. However, when ACS is caused by endoscopic manipulation, primary abdominal closure can be achieved because gas is the main cause of the increase in intra-abdominal pressure.


Comments (0)